Top 10 Facts Every Primary Care Physician Should Know About Plastic Surgery
Plastic surgery intersects with primary care more frequently than is often recognized, encompassing reconstructive, aesthetic, and hand surgery across a wide range of patient populations. Primary care physicians (PCPs) are commonly the first to evaluate patients with conditions ultimately managed by plastic surgeons, as well as the first to encounter postoperative concerns or complications. Despite this overlap, misconceptions about the scope of plastic surgery and uncertainty regarding appropriate referral, perioperative optimization, and complication recognition persist among non-surgical providers. These gaps may delay care, contribute to preventable morbidity, or place additional burden on primary care settings.
The purpose of this article is to highlight ten high-yield facts about plastic surgery that are particularly relevant to primary care practice. The “Top 10” topics were identified through a narrative review of the plastic surgery and primary care literature and refined by author consensus based on clinical experience in board-certified plastic surgery practices. Topic selection prioritized areas that (1) commonly present to or intersect with primary care, (2) have meaningful implications for patient outcomes when recognized early, and (3) are frequently misunderstood or underemphasized outside surgical specialties. By focusing on reconstructive surgery, hand and upper-extremity care, postoperative surveillance, and aesthetic procedures, this article aims to provide practical, clinically applicable guidance to support timely referral, improved interdisciplinary communication, and safer longitudinal patient care.
1. Plastic surgery encompasses reconstructive, aesthetic care, and hand surgery care.
Plastic surgery is a comprehensive surgical specialty that encompasses reconstructive, aesthetic, and hand and upper-extremity surgery, with a unifying focus on restoring function, form, and quality of life. In addition to aesthetic procedures, plastic surgeons routinely manage traumatic injuries, complex wounds, congenital anomalies, nerve compression syndromes, tendon injuries, and skin and soft tissue reconstruction. Hand surgery, including conditions such as carpal tunnel syndrome, trigger finger, Dupuytren’s contracture, and traumatic hand injuries, is a core component of plastic surgery training and practice. Primary care physicians are often the first to evaluate patients with these conditions and play a key role in initial assessment, conservative management, and timely referral to board-certified plastic surgeons certified by the American Board of Plastic Surgery.1
2. Breast surgeries are among the most commonly performed plastic surgical procedures.
Breast augmentation, reduction, and reconstruction are consistently among the top five plastic surgeries performed annually. While augmentation is typically aesthetic, breast reduction is often indicated for medical symptoms like chronic neck and back pain, shoulder grooving, or skin irritation, and it may be reimbursed if documented appropriately. PCPs frequently provide preoperative medical clearance and play a central role in managing postoperative care. Complications such as implant malposition, capsular contracture, fat necrosis, or wound dehiscence may present in a primary care setting weeks or months after surgery. A clear understanding of these procedures enables PCPs to offer reassurance when appropriate or initiate prompt referral when needed.2
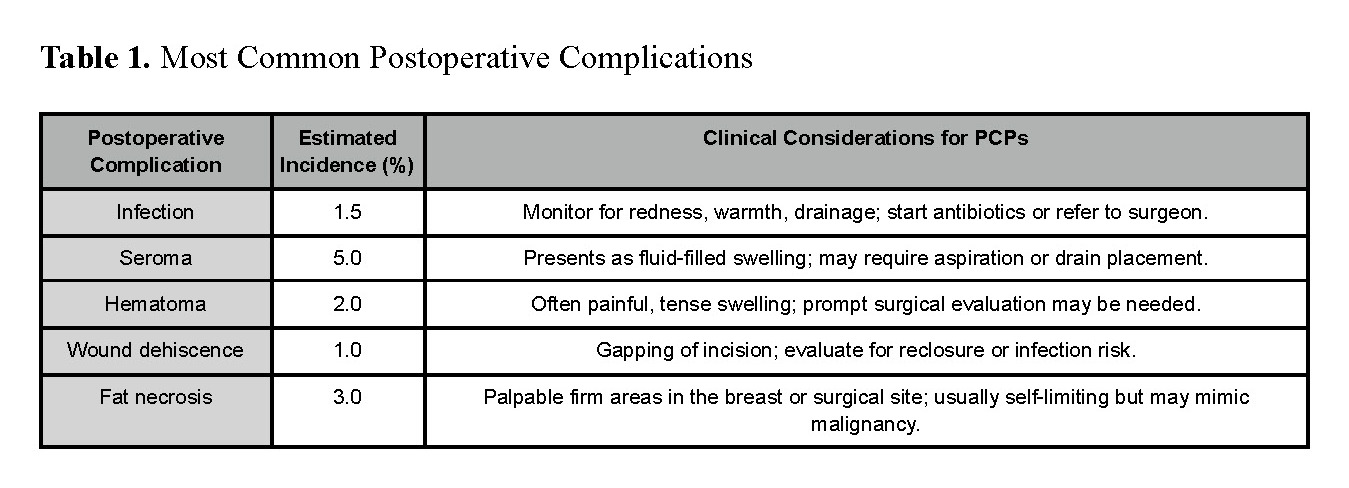
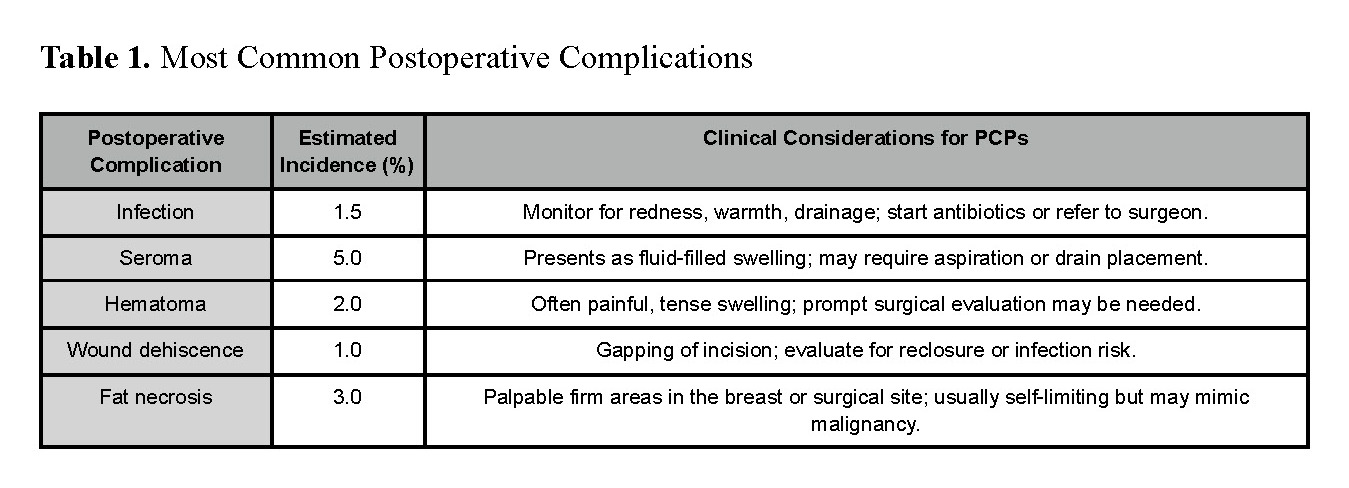
3. Postoperative complications often present first in primary care.
Patients experiencing postoperative complications may present to their PCP rather than their operating surgeon, particularly weeks to months after surgery. Common concerns include seromas, hematomas, wound dehiscence, fat necrosis, infection, and delayed healing. Distinguishing normal postoperative changes from early complications is critical. Warning signs warranting urgent referral include rapidly expanding swelling, increasing erythema, purulent or foul-smelling drainage, skin necrosis, fever, or disproportionate pain (Table 1). Familiarity with procedure-specific timelines and expected recovery patterns allows PCPs to triage appropriately and avoid delayed intervention.3
4. Preoperative risk optimization is a critical primary care responsibility.
Certain patient-related factors significantly influence postoperative healing and complication rates. Smoking, uncontrolled diabetes, obesity, poor nutrition, and steroid use are associated with delayed wound healing, surgical site infections, and dehiscence. Before elective plastic surgery, PCPs can help patients mitigate these risks by optimizing glycemic control, encouraging smoking cessation for at least 4–6 weeks pre-op, recommending weight management strategies, and addressing any nutritional deficiencies. These preventive efforts are particularly important for patients undergoing abdominoplasty, breast reconstruction, or facial procedures where tension on incisions is high and healing complications can affect long-term outcomes.4
5. Hand and upper-extremity conditions frequently require plastic surgery referral.
Hand pathology represents a significant and often under-recognized portion of plastic surgery practice. Conditions such as carpal tunnel syndrome, trigger finger, Dupuytren’s contracture, tendon lacerations, nerve injuries, and complex hand trauma frequently present initially to primary care. Early recognition of red flags, such as loss of motor function, sensory deficits, ischemia, open fractures, or worsening neuropathy, is essential to prevent permanent disability. PCPs play a key role in initiating conservative management when appropriate (e.g., splinting, NSAIDs, activity modification) while ensuring timely referral for surgical evaluation when symptoms persist or functional compromise is present.5
6. Informed referral protects patient safety in elective plastic surgery.
Given the increasing availability of cosmetic procedures outside traditional medical settings, PCPs are often asked to advise patients seeking aesthetic care. Referral to surgeons certified by the American Board of Plastic Surgery or American Board of Facial Plastic and Reconstructive Surgery ensures appropriate surgical training, credentialing, and adherence to safety standards. PCPs should encourage patients to verify board certification, hospital privileges, and postoperative care pathways, particularly for procedures requiring anesthesia or implantable devices. Informed referral reduces the risk of complications managed downstream in primary care settings.6
7. Injectables like fillers and neuromodulators are not without risk.
While dermal fillers and botulinum toxin injections are marketed as low-risk, non-surgical treatments, they can have serious complications when administered improperly. Adverse outcomes include vascular occlusion, skin necrosis, granulomas, and even irreversible blindness. Patients may present to their PCP with complaints of facial pain, discoloration, nodules, or visual disturbances hours or days after treatment. PCPs should be able to recognize these red flags and refer patients to specialists, ideally plastic surgeons or dermatologists, who are trained to manage complications of cosmetic injectables.7
8. Plastic surgeons are integral to skin cancer management and reconstruction.
When skin cancers occur in cosmetically or functionally sensitive areas, such as the nose, lips, eyelids, or scalp, dermatologic excision may leave defects requiring flap or graft reconstruction. Plastic surgeons are skilled in preserving function and aesthetics in these high-risk areas. PCPs should biopsy suspicious lesions promptly and coordinate referrals to dermatology and plastic surgery as needed. This coordination is particularly important for recurrent cancers, large lesions, or those with poorly defined borders. Collaboration across specialties improves cosmetic outcomes and reduces the need for revisions.8
9. Early referral improves outcomes for pediatric plastic surgery patients.
Many congenital anomalies, such as cleft lip/palate, craniosynostosis, syndactyly, and prominent ears, require multidisciplinary evaluation and timely surgical correction. Delays can negatively impact feeding, speech, psychosocial development, or craniofacial growth. PCPs are often the first to detect these anomalies during newborn and well-child visits. Prompt referral to a craniofacial team or pediatric plastic surgeon allows for coordinated care with speech therapy, orthodontics, and otolaryngology, ensuring the best functional and aesthetic outcomes.9
10. Some plastic surgery procedures require long-term surveillance and follow-up.
Patients with breast implants, especially after reconstruction, require periodic imaging to screen for asymptomatic rupture. The U.S. FDA recommends MRI or high-resolution ultrasound 5–6 years after placement and every 2–3 years thereafter. Additionally, patients should be monitored for late complications such as capsular contracture, implant malposition, or rare conditions like breast implant-associated anaplastic large cell lymphoma (BIA-ALCL). PCPs should document implant history in the patient’s medical record and educate patients about signs and symptoms that warrant further evaluation.10
Plastic surgery intersects with primary care across the lifespan, from congenital anomalies and hand injuries to cancer reconstruction and long-term implant surveillance. Having a working understanding of the breadth of plastic surgery practice including hand surgery, reconstructive care, and aesthetic procedures, empowers PCPs to optimize preoperative health, recognize complications early, and facilitate timely referral. Strengthening this interdisciplinary interface ultimately improves patient safety, functional outcomes, and continuity of care.