
Report
A 32-year-old, G6P0242, African American female with a history of complete abortion (April 2025), latent syphilis, diabetes mellitus, previous intravenous drug use (cocaine), hypertension, and tobacco use was transferred to a Mississippi community hospital for worsening shortness of breath for greater than 30 days.
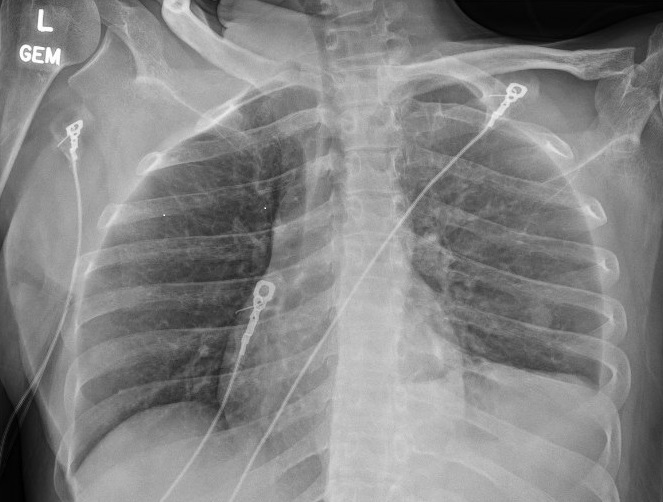
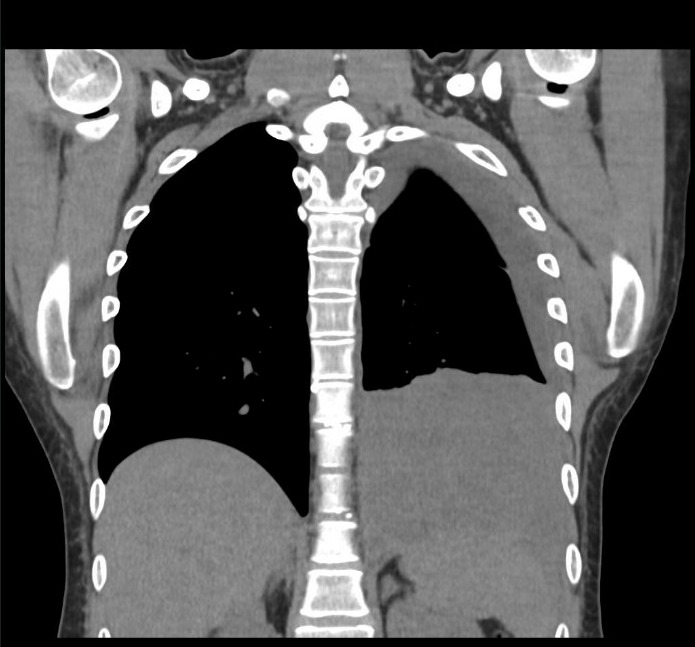
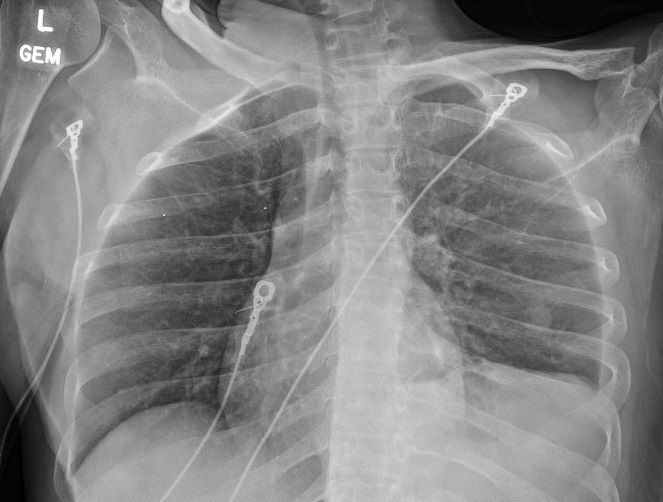
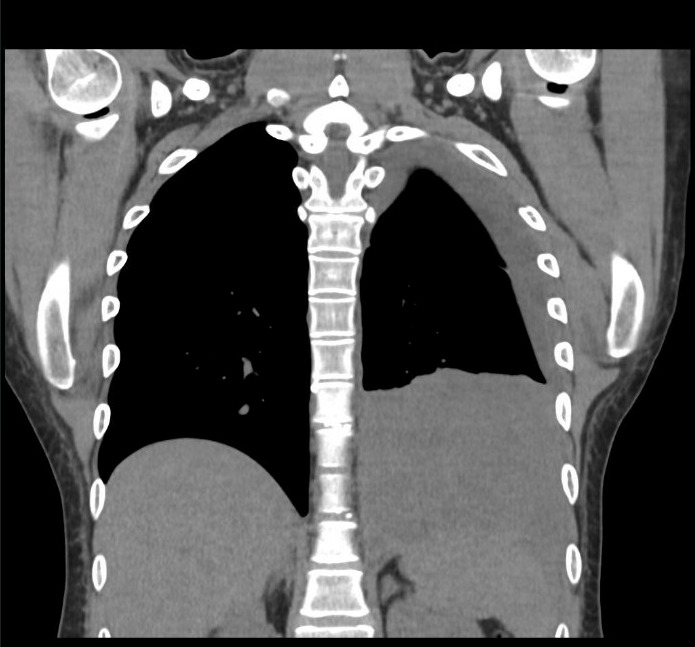
A chest x-ray (figure 1) showed new left lung consolidation with left pleural effusion. Chest computed tomography (CT) scan (figures 2 and 3) and bronchoscopy revealed acute necrotizing pneumonia and growth of anaerobic bacteria (Prevotella buccae). Labs on admission showed abnormal findings, including leukocytosis (20,000), hyponatremia (126 mmol/L), elevated procalcitonin (36.23), and positive Methicillin-Resistant Staphylococcus aureus (MRSA) on nares.

Intravenous cefepime and vancomycin were administered, and interventional radiology (IR) was consulted for thoracentesis. The IR thoracentesis failed, and a repeat chest CT scan showed minimal improvement in the left lower lobe pneumonia. Additionally, a new right lung consolidation and a right pleural effusion were noted on CT. Intravenous piperacillin-tazobactam was started and later switched, due to worsening clinical symptoms, to intravenous meropenem.
The patient’s hospital course remained complicated despite IV antibiotic treatment. Cardiothoracic surgery was consulted and performed a left thoracotomy, lower left lobectomy, and decortication. Results showed a necrotic, cavitary left lower lung lobe with purulent drainage into the posterior mediastinum, severe diaphragmatic adherence, and histopathology consistent with empyema. Postoperatively, metronidazole was added due to persistent leukocytosis. The patient was discharged after six weeks in hospital, continuing oral linezolid, metronidazole, and fluconazole for an additional six weeks.
Concurrently, the patient was found to have a positive Rapid Plasma Reagin (RPR) titer of 1:256 during this hospitalization. This titer, along with increased confusion, prompted the infectious disease team to treat her with continuous intravenous penicillin due to concerns about neurosyphilis. After cerebrospinal fluid analysis showed a negative Venereal Disease Research Laboratory (VDRL) test, intravenous penicillin was discontinued, and she received a single dose of 2.4 million units of intramuscular Penicillin G Benzathine to treat early latent syphilis.
Patient History of Syphilis
During the May 2025 hospitalization, the patient had an incidental finding of 1:256 RPR titer and was diagnosed with latent syphilis. Previously, during an emergency department visit in November 2024, the patient was found to be six weeks pregnant with a RPR titer of 1:32. The patient later miscarried this pregnancy in April 2025 at 25 weeks of gestation.
In March 2023, the patient was diagnosed with late latent syphilis during her fifth pregnancy. Her RPR titer was 1:128. This pregnancy resulted in the preterm birth of a baby with congenital syphilis in April 2023. The patient received two doses of 2.4 million units of penicillin G Benzathine and was instructed to get a third dose as an outpatient. However, there is no record of her receiving the third dose as an outpatient in her chart or in the Mississippi Department of Health’s records. She reported that her partner was evaluated for syphilis, but it is unclear if he was diagnosed or treated. From March 2023 to May 2025, there were no intervening negative RPR results. Her previous history shows a negative syphilis test in 2020 during her first live birth.
Social Determinants of Health Impact
After her baby was born with congenital syphilis, the patient, along with the baby’s father and sibling, moved in with the baby’s paternal grandmother. Three months later, the house burned down, leaving them homeless. She lived in a car for nearly a year while her children stayed with their maternal grandmother, who would not let her partner into her home. During this time, emergency departments were her primary care providers because she lacked health insurance. She had repeated visits and was prescribed medications, but her health-related social needs were largely unaddressed. She was uninsured, homeless, and unemployed, and remained with her partner despite uncertainty about whether he had been treated for latent syphilis.
Discussion
This patient’s history of latent syphilis resulted in the delivery of a baby with congenital syphilis. Congenital syphilis occurs with vertical transmission from an infected mother to the baby and could cause lasting health problems if untreated.1 Despite penicillin being an easily accessible treatment, congenital syphilis has become a public health concern in Mississippi. The number of congenital syphilis cases in Mississippi has risen significantly from 3 cases in 2019 to 131 cases in 2023.2 In 2022, Mississippi ranked 6th in the nation for congenital syphilis cases, with a reported rate of 207.6 per 100,000 live births.3 Mississippi has increased efforts in reporting syphilis, especially during pregnancy, mandating screening during the first and third trimesters in 2023.4
Research shows that unfavorable SDOH can contribute to adverse patient outcomes. For example, a California study found that individuals experiencing housing insecurity, financial struggles, and limited access to healthcare experienced higher rates of syphilis.5 Our patient’s situation is like that of the participants. She was found on multiple visits to have a positive RPR titer. This patient also had a lengthy hospitalization, and, at discharge, she lived with a cousin of her partner and obtained medications through a hospital-sponsored indigent fund.
Healthcare providers can improve health outcomes by identifying and addressing specific health-related social needs stemming from undesirable SDOH. During our patient’s repeat emergency department visits, her social needs were not adequately addressed. Emergency departments (EDs) are ideal settings for screening for health-related social needs, especially given the availability of social resources within hospitals. However, some EDs face barriers that hinder providers from addressing health-related social needs, such as limited staff and time.6 Healthcare facilities should continue to support EDs in their efforts to address patients’ social needs for better health outcomes.
Conclusion
This case report details a patient’s complex hospital course of empyema and syphilis co- infection. The patient’s syphilis history, which resulted in congenital syphilis in their baby, stems from undesirable social determinants like housing insecurity and no health insurance, resulting in unmet social needs. Addressing the patient’s health-related social needs could improve health outcomes. Emergency departments have the potential to be crucial places to address needs with the support of their facilities.