Introduction
Since 1981, more than 700,000 people in the United States have died from HIV, and another 1.2 million are currently living with HIV. Despite having the ability to treat persons living with HIV and to prevent others from acquiring it, 38,000 Americans are newly diagnosed each year.1 The status of the HIV epidemic in Mississippi also remains poorly controlled. There are currently 9,915 people in Mississippi living with HIV (401 cases/100K). The rate of new diagnoses in 2023 was 18 cases/100K in Mississippi, with the national average being 13 cases/100K. Additionally, Mississippi has a higher mortality rate than the national average (8 per 100K versus 7 per 100K).2
The importance of early diagnosis and treatment of HIV with antiretroviral therapy has been clearly outlined in the literature.3 Starting antiretroviral treatment early not only provides better long-term health outcomes for patients living with HIV, but it also lowers the risk of transmission to others.4 Of the people living with HIV in Mississippi, 52.5% have been linked to care, 49.9% have received either CD4 count or viral load testing, and only 33.6% have achieved viral suppression. Mississippi has a PrEP-to-need ratio (PnR) of 4.0, indicating that PrEP use does not adequately meet the need for HIV prevention.
Purpose
Mississippi lies well below the national average in the percentage of persons living with HIV who have been linked to care, engaged in care, and achieved viral suppression. This status likely has a profound impact on the high new diagnosis rate, high mortality, and low PnR seen in Mississippi. This study aims to assess the opinions of healthcare professionals on the likely practices and strategies for providing optimal HIV care, to identify barriers preventing persons living with HIV from connecting with care, and to formulate strategies to improve the quality of care for those living with HIV in our state.
Methods
Methods Approach
A 19-question survey, developed through a review of relevant HIV care literature and refined by an expert panel of clinicians and program administrators, was administered via Research Electronic Data Capture (REDCap) to healthcare professionals in Mississippi. Data collection began on April 1, 2024, and concluded on July 1, 2024. The survey received responses from 173 healthcare professionals. The quantitative analysis aimed to assess healthcare professionals’ knowledge of the Ryan White Part B Ending the HIV Epidemic (EHE) Program and how they incorporate its resources into their clinical practice. Additionally, the survey explored healthcare professionals’ perceptions of current HIV testing and treatment practices in Mississippi.
The quantitative survey instrument included multiple-response selections and another option, allowing respondents to write in answers to capture qualitative insights. The target population for this study was healthcare professionals in the state of Mississippi. The questions assessed healthcare professionals’ views and confidence regarding HIV care, while the multiple-response format and Other options measured awareness and utilization of program resources. Open-ended responses were incorporated to enable further elaboration on key issues. The survey instrument was created in REDCap, and the link sent was to physicians in Mississippi who were and are also engaged in some form of HIV work, data processing, and patient care. They were asked to complete the survey while timing themselves to determine the average length of time it took to complete the form. They were also asked to respond to the survey with suggestions and recommendations on necessary edits that should be implemented in the instrument. Their responses were reviewed and structured into the final survey that was sent out to the participants. These physicians and their responses were not included in the final survey responses used for the study.
Participants
173 healthcare professionals contacted by the Mississippi State Department of Health (MSDH), through the Mississippi State Medical Association (MSMA), and the Mississippi Medical and Surgical Association (MMSA), completed surveys. In this study, a healthcare professional refers to any trained and licensed individual who offers medical services to patients in Mississippi.
Data Collection
After approval was granted from the Mississippi State Department of Health’s Institutional Review Board (IRB), data collection began. A nineteen-question REDCap survey was sent to Mississippi healthcare professionals. A quantitative analysis was performed using REDCap to analyze the responses submitted by the healthcare professionals.
Recruitment
This Ryan White EHE study focuses on healthcare professionals affiliated with the MSMA and MMSA. When conducting research for the Ryan White EHE healthcare professional-only study, it is crucial to define precise inclusion and exclusion criteria to maintain the study’s focus on healthcare professionals and avoid including patient data. Criteria for inclusion may involve healthcare professionals actively engaged in caring for patients in Mississippi. Exclusion criteria may include healthcare professionals who do not have direct patient interaction or are not licensed to practice in the state. The healthcare professionals who participated in the quantitative survey were recruited through a collaboration between MSDH, MSMA, and MMSA. MSMA and MMSA are comprised of nearly 5,000 physicians and medical students.5 These professionals were recruited through multiple channels, such as direct email, their weekly correspondence, and a conference newsletter at the annual MSMA conference and the annual MMSA conference. Over 500 healthcare professionals were contacted, with participant recruitment facilitated through affiliations with MSMA and MMSA to maximize accessibility. With this method of recruitment, we engaged in convenience sampling. According to Simkus,6 convenience sampling is a non-probability sampling method where data is collected from participants who are easily accessible to the researcher. Within the scope of the inclusion criteria, we used healthcare professionals who were easily accessible. Due to conflict in schedules and time constraints of the researchers, this manner of usage was the best option for maximizing responses.
Survey Data
Following approval from the Mississippi State Department of Health’s Institutional Review Board (IRB), data collection commenced. Healthcare professionals were recruited for the quantitative survey through a collaboration with the Mississippi Medical Association (MSMA). MSMA facilitated recruitment via multiple channels, including direct email invitations, weekly newsletters, and a conference newsletter distributed at the Annual MSMA Conference. Additional participants were recruited through the Mississippi Nursing Association and the Mississippi Medical and Surgical Association (MMSA).
A nineteen-question REDCap survey was administered and analyzed using REDCap’s built-in statistical tools to calculate percentages and frequencies. The target sample size for the Mississippi State Medical Association (MSMA) study was 214.
Survey Administration
Over 500 healthcare professionals were contacted, with participant recruitment facilitated through affiliations with MSMA and MMSA to maximize accessibility. Basic demographic data collected included healthcare professional phone number, email, credentials, specialty, and county of practice. A total of 173 responses were received, falling short of the target sample size due to uncontrollable factors such as healthcare professionals’ demanding schedules and limited available resources. The survey was conducted from April 1, 2024, to July 1, 2024. This timeframe was selected to align with the researcher’s practicum experience. This limitation may impact the generalizability of findings and introduce potential response bias, necessitating careful consideration in the interpretation of results. Since REDCap was used to deliver the survey, the response limit feature was used to prevent the number of times a survey could be accessed.
Ethical Considerations
Before the initiation of data collection, approval was granted by the Mississippi State Department of Health’s IRB. During the data collection phase, anonymity and confidentiality were considered. The survey only collected the healthcare professionals’ email addresses. Their names and place of employment were not collected in the survey. All the data was stored in REDCAP, with only the MSDH/Ryan White/Ending HIV Epidemic staff and program interns having access to the data stored in REDCap.
Statistical Analysis
Quantitative analysis of survey responses was conducted using REDCap’s built-in analytical tools and exported for further statistical examination. There were no missing items in the survey. All the respondents were required to complete all the questions in the survey to complete the questionnaire. Descriptive statistics were calculated to identify trends, gaps in healthcare professional knowledge, and barriers to implementing HIV care strategies. Responses to the questions were coded numerically and analyzed for central tendency and variability. The responses were analyzed using frequency distributions and cross-tabulations to determine patterns in healthcare professional responses. Exploratory analyses were considered for the data analysis method. However, a descriptive analysis method was selected to describe patterns, distributions, and associations without drawing causal conclusions or altering conditions of the study. Missing data were excluded from the analysis by the REDCAP software.
Results
Survey Data
A total of 173 participants completed the survey, including 92 physicians, 71 advanced practitioners (Advanced Practice Nurses, physician assistants), and 10 other professionals (clinic managerial staff, dentists, and four of unknown clinical designation).
Detection and Diagnosis
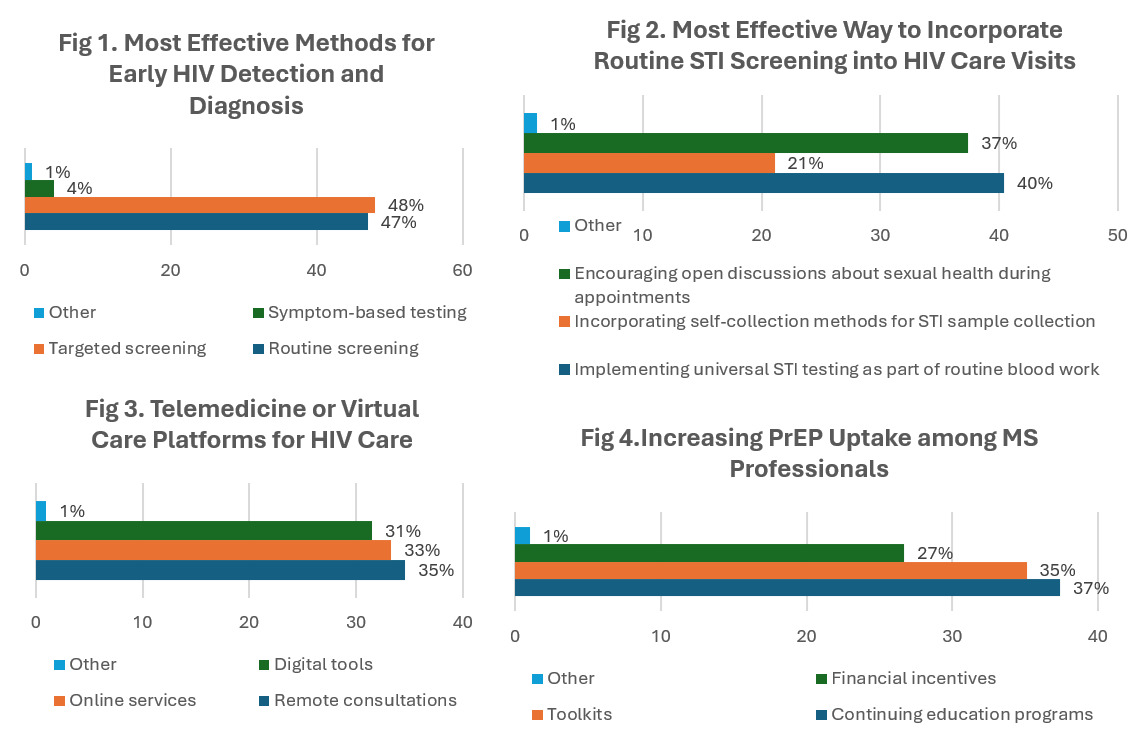
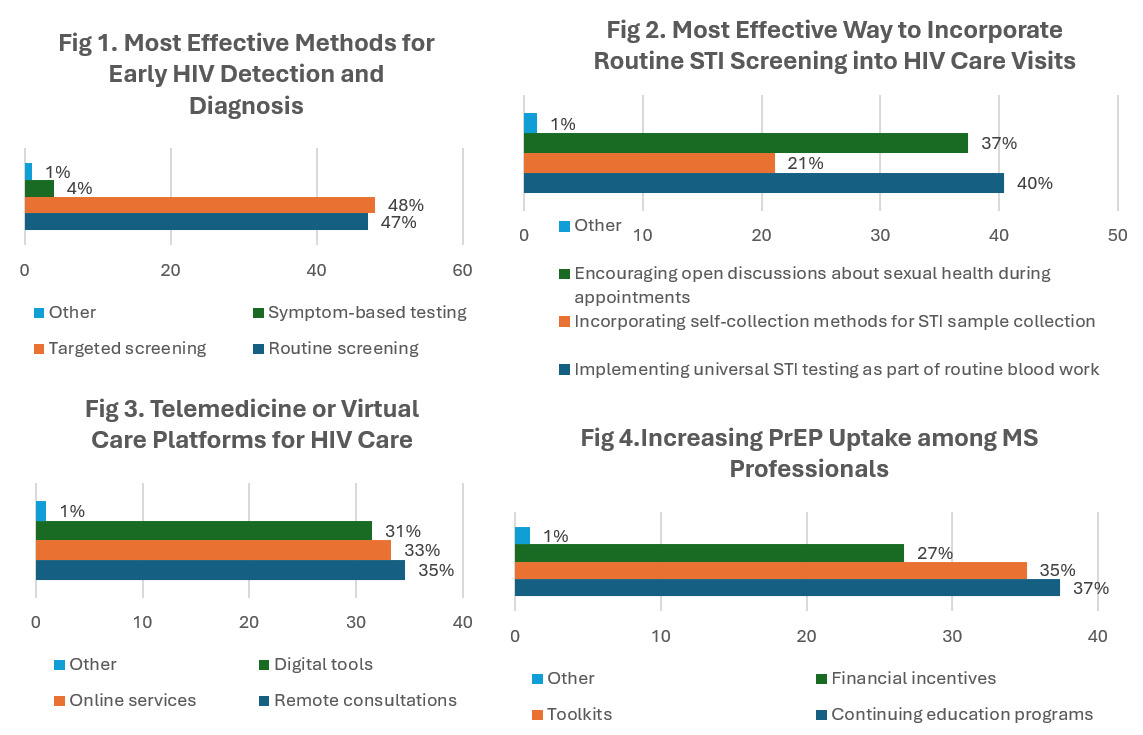
As shown in Figure 1, the data indicate that most healthcare professionals concluded that the effective methods for early HIV detection and diagnosis in Mississippi were targeted screening based on high-risk behaviors or demographics (122, 70.5%). The results were closely followed by routine screening with 119 responses.
As shown in Figure 1, the data indicate that most healthcare professionals in Primary care clinics (153, 88.4%) should be prioritized for increasing access to HIV testing services in Mississippi. The results revealed that healthcare professionals should implement universal STI testing as part of routine blood work (144, 83.7%) is the most effective way to incorporate routine STI screening into HIV care visits. (Figure 2). The data indicate that most healthcare professionals should be conducting regular laboratory testing as part of annual check-ups (153, 89.0%). This method can be instrumental in HIV care settings to evaluate treatment efficacy while monitoring viral suppression rates. The data indicate that most healthcare professionals deemed public awareness campaigns to be the likely source to use for promoting acceptance and understanding (153, 88.4%) to reduce HIV-related stigma and discrimination in healthcare settings.
Telehealth
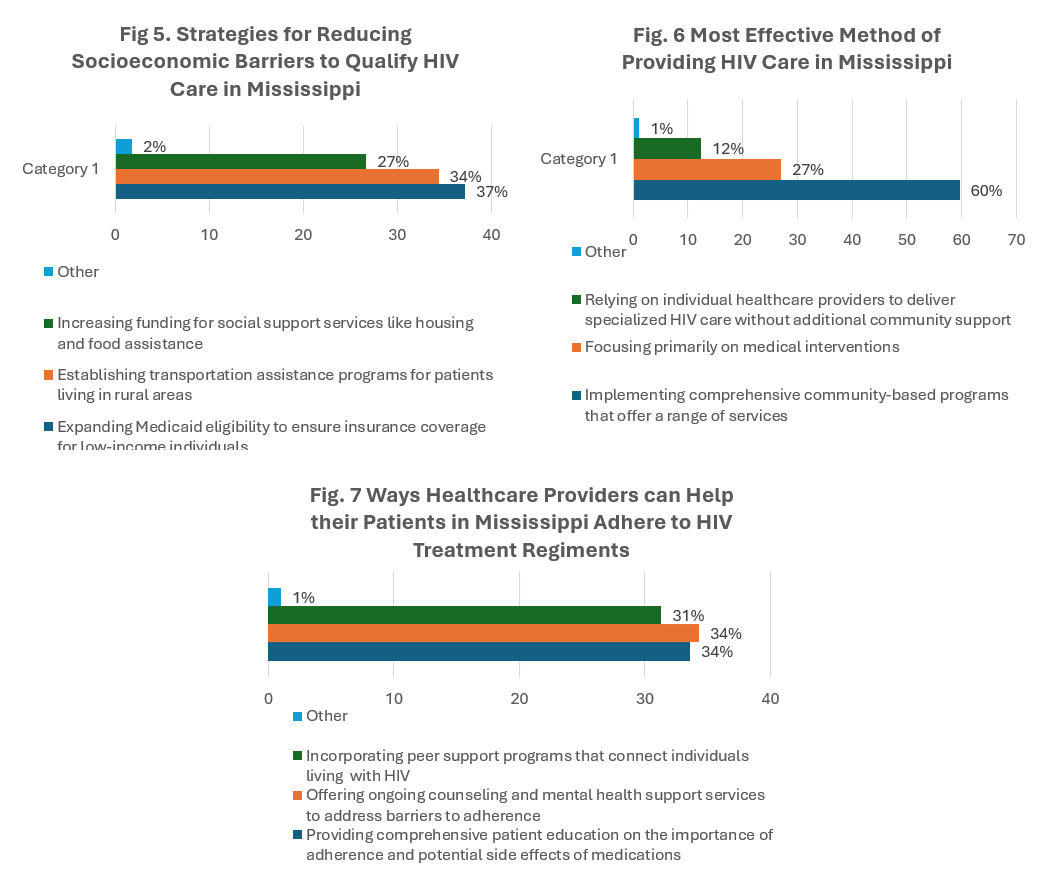
As shown in Figure 3, the data indicate that most healthcare professionals providing remote consultations for routine follow-up visits (155, 89.6%) via telemedicine or virtual care platforms should be included in HIV care in Mississippi.
As shown in Figure 3, the data indicate that most healthcare professionals agree that remote consultations (telehealth) are the most likely approach (155 responses) to overcoming geographic barriers and increasing retention in care, followed by online services (149 responses) and digital tools (141 responses).
The data indicate that most healthcare professionals expressed that men who have sex with men (MSM) (136, 79.1%) should receive priority attention when implementing targeted interventions to address HIV disparities in Mississippi.
Pre-exposure Prophylaxis
As shown in Figure 4, the data indicate that most healthcare professionals agreed that offering continuing education programs on PrEP prescribing guidelines (143, 83.1%) will increase PrEP uptake among Mississippi healthcare Professionals.
The data indicate that most healthcare professionals agree that expanding access to pre-exposure prophylaxis (PrEP) medications among high-risk individuals (156, 90.2%) shows the greatest potential for reducing new HIV infections in Mississippi.
As shown in Figure 4, the data indicate that most healthcare professionals agree that lack of awareness among healthcare professionals and community members (134, 77.5%) is the most significant barrier to receiving PrEP (Pre-Exposure Prophylaxis) in Mississippi.
Health Insurance Coverage
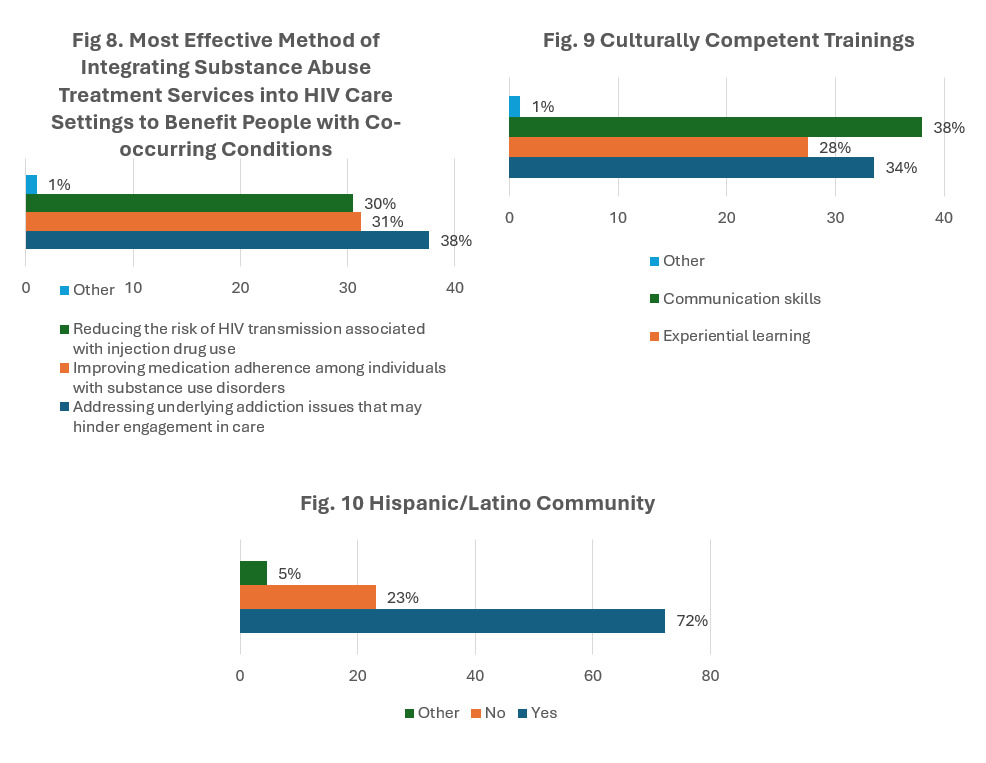
The data indicate that most healthcare professionals agree that expanding Medicaid eligibility to ensure insurance coverage for low-income individuals (146, 84.9%) can be used to reduce socioeconomic barriers to quality HIV care in Mississippi. (Figure 5)
Programs and Services
The data indicate that most healthcare professionals agree that implementing comprehensive community-based programs that offer a range of services, including testing, treatment, prevention education, and support (159, 93.0%) is the most effective method of providing HIV care in Mississippi. (Figure 6)
The data indicate that most healthcare professionals agree that encouraging the involvement of people living with HIV in program planning and decision-making processes (137, 79.2%) should be effectively addressed within healthcare settings in Mississippi.
The data indicate that most healthcare professionals agree that offering ongoing counseling and mental health support services to address barriers to adherence (147, 85.0%) can help their patients adhere to HIV treatment regimens. (Figure 7)
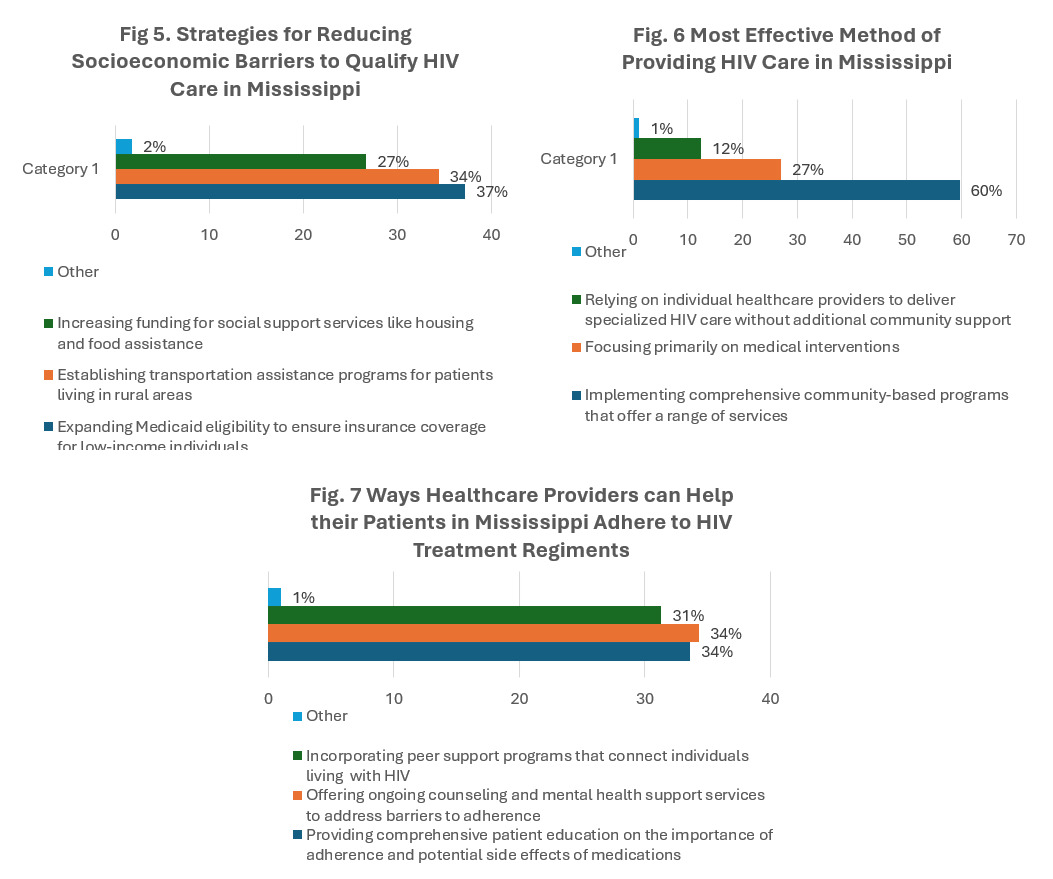
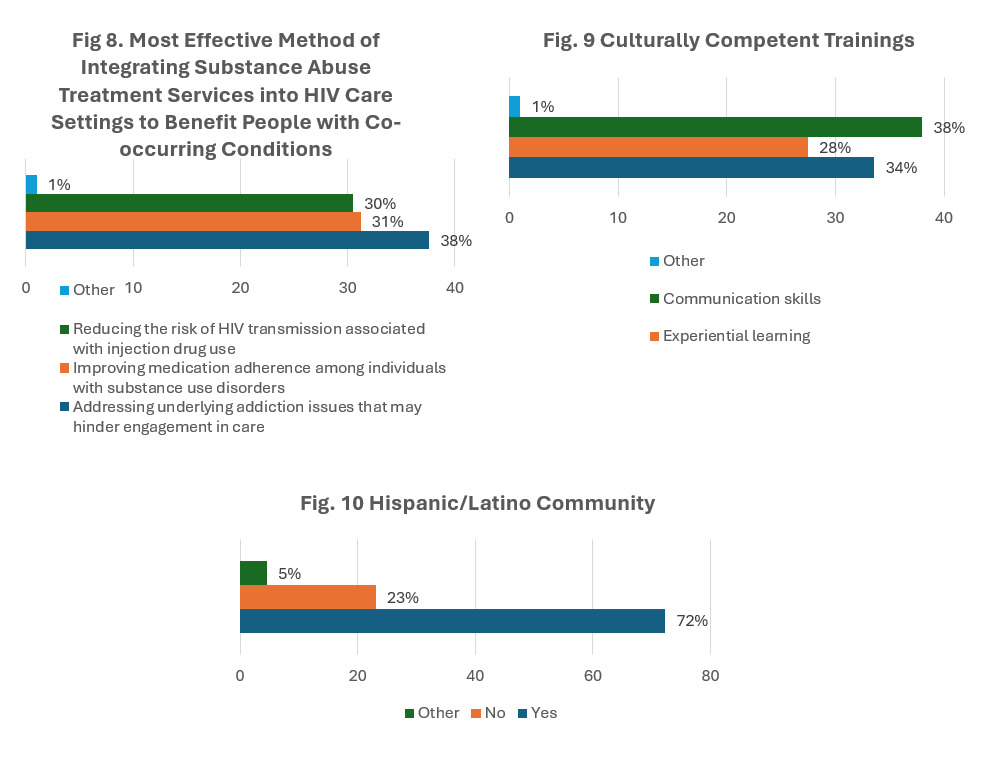
The data indicate that most healthcare professionals agree that addressing underlying addiction issues that may hinder engagement in care (148, 86.0%) is the most effective method of integrating substance abuse treatment services into HIV care settings to benefit people with co-occurring conditions. (Figure 8)
The data indicate that most healthcare professionals agree that establishing collaborative referral networks for comprehensive care (151, 87.8%) among healthcare professionals, community organizations, and public health agencies should be strengthened to improve HIV care in Mississippi.
As shown in Figure 9, the data indicate that most healthcare professionals agree that communication skills (131, 76.2%) can be incorporated into healthcare curricula to better serve culturally diverse populations affected by HIV in Mississippi, followed by case studies and workshops with 116 responses and experimental learning with 95 responses.
Hispanic Populations and HIV Care
As shown in Figure 10, of the healthcare professionals completing the survey, 125 (72.3%) serve the Hispanic/Latino community.
Discussion
The survey findings indicate a clear consensus among healthcare professionals regarding pivotal aspects needed for improving HIV prevention, detection, and treatment in Mississippi. The focus on targeted screening and universal STI testing emphasizes the significance of proactive and coordinated approaches in HIV detection, prioritizing vulnerable populations, and consistent inclusion across healthcare settings. The prioritization of primary care clinics as key venues for expanding testing access indicates their accessibility and value in mitigating health disparities. Public awareness campaigns were proposed as an intervention strategy to mitigate stigma, addressing the significance of eliminating cultural and societal obstacles to improve acceptance and health outcomes.
The significant support for telehealth projects signifies recognition of their ability to eradicate geographic and logistical barriers to healthcare access. Remote consultations and telehealth programs can enhance retention in care and facilitate constant monitoring of treatment outcomes, particularly in rural or underserved areas. The promotion of targeted treatments for men who have sex with men (MSM) demonstrates a commitment to tackling disparities within this demographic, which is disproportionately affected by HIV. The findings indicate an intricate awareness of the necessity for innovative and inclusive techniques to enhance accessibility and equity in HIV care, as is conveyed in the intent behind the Ending the HIV Epidemic Initiative.
The survey reveals significant gaps and prospective opportunities in HIV prevention and treatment. The advocacy for the extension of PrEP access and educational campaigns highlights its significance in decreasing new infections.7 The reported deficiency in awareness among healthcare professionals and community members represents a barrier to effective implementation. The focus on comprehensive community-based programs and culturally sensitive communication points out the need to tailor care to address the diverse needs of Mississippi’s population, particularly the Hispanic/Latino community.8 The emphasis on Medicaid expansion, collaborative referral networks, and integrated substance addiction treatment confirms the importance of systemic reforms to address socioeconomic and behavioral health barriers, which will ensure that HIV care is comprehensive, accessible, and sustainable.9
The findings of this survey hold considerable implications for academia, particularly in the fields of public health, healthcare delivery, and health policy.10 The focus on targeted screening and routine integration of STI testing into primary care emphasizes the necessity for additional research on optimal practices for implementing these initiatives across various healthcare environments. Researchers should evaluate the effectiveness of targeted screening in high-risk populations and identify specific demographic or behavioral markers that provide the greatest diagnostic impact. Moreover, the public health curriculum should integrate these findings to emphasize the significance of systematic methods for early identification and prevention in mitigating HIV transmission.10
The endorsement of telehealth and virtual care platforms signifies a growing need for research on the efficacy and scalability of telemedicine in HIV care, particularly in rural and underserved areas.11 Researchers could investigate the long-term effects of telehealth initiatives on patient retention, virus suppression, and health outcomes. The prioritization of interventions for men who have sex with men (MSM) underscores the need for research into culturally competent and community-specific strategies to reduce disparities in HIV care. The findings can guide the development of evidence-based interventions tailored to the distinctive needs of marginalized populations.
The findings surrounding PrEP adoption and community-based programs indicate healthcare professional and community awareness limitations, suggesting possible avenues for scholarly inquiry into educational campaigns and public health initiatives.7 Researchers can investigate the effects of continuing education programs on the prescribing behaviors of healthcare professionals to assess the effectiveness of community-based initiatives in increasing awareness and reducing stigma. The focus on Medicaid expansion and collaborative referral networks suggests the need for policy-based research to address systemic barriers to care.9 Researchers may examine the impact of structural reforms on health equity and outcomes, thereby augmenting the comprehension of strategies that improve HIV care and prevention in socioeconomically underserved areas in Mississippi.
Limitations
Similar to others, this study has its limitations. This study was originally a mixed-methods study. Due to a lack of participants in the interview portion of the study, we focused solely on the quantitative results. With the exclusion of the qualitative portion, this manuscript has less focus on understanding the context of the problem as it relates to responses from healthcare professionals.12 The data collection method used poses limitations as well. Though surveys are one of the most used quantitative research techniques, the reliability of the survey is dependent on its structure and the accuracy of the participants’ responses.12 Another limitation is that the sample size was not reached. We met 81% of the 214-sample size goal. Not reaching the sample size has limitations of its own. Having a smaller sample size challenges the reliability and validity of a study.13 Another limitation that should be noted is that our survey did not capture the specific specialties of the respondents. Braam et al supports that this may be a limiting factor within the study because when physicians specialize, they take on professional identities and behaviors like their colleagues and supervisors.14 With our chosen methods, we were not able to capture a more in-depth understanding of the complexities per specialty.
Interpretations
The limitation surrounding the abbreviated timeframe in which the survey was administered may impact the generalizability of findings. This limitation could also introduce potential response bias, necessitating careful consideration in the interpretation of results.
Generalizability
Generalizability refers to the degree to which researchers can apply the results of a study to a broader context.15 The results of this study could be generalizable with some modifications to adhere to populations. For example, similar studies could survey healthcare professionals regarding telehealth, health insurance coverage, and programs and services for other diseases and ailments of interest.
Recommendation for Future Research
Based on the limitations of this study, there are recommendations for future research. First, a qualitative research design should be completed and included. Structured interviews to follow up on the responses would allow the researcher to gather and compare responses.12 Qualitative research allows for a more in-depth understanding of the problem. This type of research also allows for higher flexibility and exploratory analysis.12 The inclusion of a qualitative research portion could eliminate conjecture regarding the responses labeled as “other”. Future researchers could allow the survey to be open and available to healthcare professionals and/or participants. Time constraints from both parties limited the time the survey was open. In a future study, researchers could offer this survey to persons living with HIV. With this study only receiving opinions from the healthcare professionals, including the affected population, could provide different perspectives and insight. Researchers in the Netherlands conducted in-depth interviews with persons living with HIV who received a “late” diagnosis.16 Those interviews aimed to understand the possible factors and reasons for the delayed diagnosis. Considering their approach, the opportunity for future research could incorporate an examination of the social determinants of health (SDOH). SDOH, as defined by the Centers for Disease Control and Prevention (CDC), is the environment in which a person is born, works, lives, and plays. The CDC also informs that SDOH affects a “wide range of health, functioning, and quality of life outcomes and risks”.17 Persons living with HIV who report SDOH indicators are more likely to miss appointments, experience barriers to HIV care and adherence, and reach viral suppression.18
Conclusion
The findings of this study underscore the critical gaps and opportunities in HIV prevention and treatment in Mississippi. Healthcare professionals identified targeted screening, telehealth expansion, and comprehensive community-based programs as pivotal strategies for improving access to care and achieving better health outcomes, which incidentally are the areas of focus of the Mississippi Ryan White Part B Ending the HIV project. Moreover, the emphasis on culturally sensitive communication and addressing systemic barriers, such as Medicaid expansion, highlights the multifaceted approach needed to combat HIV disparities, accentuating the need for innovative and non-traditional strategies in HIV care and treatment.
To translate these insights into actionable steps, policymakers should prioritize integrating targeted screening and universal STI testing into primary care. Expanding telehealth initiatives and PrEP accessibility will help address geographic and socioeconomic barriers. Additionally, fostering collaborations among healthcare professionals, community organizations, and public health agencies can create robust referral networks and enhance service delivery.
This study reaffirms the significance of the innovative strategies of the Ending the HIV Epidemic initiative in tackling HIV care challenges. By addressing gaps in awareness and promoting equity-focused interventions, thereby expanding access to HIV care, Mississippi has the potential to set a precedent in the nation on how to end the HIV epidemic for other states grappling with similar disparities. Future research could delve deeper into the social determinants of health and include qualitative insights to complement these quantitative findings, ensuring a comprehensive understanding of HIV care dynamics. This manuscript draft follows the guidelines of the Consensus-Based Checklist for Reporting of Survey Studies (CROSS).19