Introduction
Head and neck cancers pose a significant health challenge, now with over 70,000 new cases and over 16,000 deaths annually in the United States.1 Among these, laryngeal cancer represents a significant subset, particularly in Mississippi, which reports the highest incidence in the country at 4.6 cases per 100,000 people.2 Timely identification of laryngeal cancer is crucial for improving patient outcomes, as delayed diagnosis is associated with worse prognosis.3 In the United States, the overall five-year relative survival rate for laryngeal cancer is 61.6%, which rises to 79.4% when it is diagnosed at an early stage.4 This rise emphasizes the need for heightened awareness and early detection strategies, particularly in high-incidence areas, to enhance treatment success and patient survival rates.
Access to preventive healthcare is significantly influenced by the presence of a regular medical home, primarily managed by primary care providers (PCPs).5,6 It is estimated that otolaryngic issues comprise 20% of adult general practice complaints.7 This aspect is especially crucial in head and neck cancer management, as PCPs often serve as a patient’s first point of contact prior to otolaryngology evaluation. Reid, et al., demonstrated that continuity of care was directly associated with an earlier diagnosis of head and cancer cancers.8 Previous studies have shown that otolaryngology is neither emphasized in medical school9–12 nor in primary care postgraduation education.13,14 It has been shown that the level of otolaryngology expertise among PCPs is limited, and there is a known paucity of information regarding education in continuing medical education (CMEs).7 This unexpected figure highlights a need for more comprehensive and uniform otolaryngology education within primary care training programs. This study seeks to assess the knowledge and confidence of PCPs related to identifying the signs and symptoms of laryngeal and other head and neck cancers in a state with high incidence of these cancers. Our secondary aim is to evaluate PCP interest in further education on head and neck cancers with the aim of gathering data to inform future educational programs.
Materials and Methods
A twenty-two-question survey was designed after Institutional Review Board approval was obtained at the University of Mississippi Medical Center. PCPs were identified through the Mississippi Board of Medical Licensure as practicing internal medicine or family medicine physicians (MD/DO). A list of available email addresses was obtained, and providers without listed emails were contacted via mailed letters containing a QR code linking to the survey. The survey was distributed to 545 PCPs in the five counties of Mississippi with the highest incidence of laryngeal cancer (Hinds, Warren, Forrest, Washington, and Leflore) using institutional data on laryngeal cancer patients diagnosed from 2013-2020. The survey was open from March 2022 until May 2022. Participants received compensation in the form of a gift card for survey completion. The questionnaire (Appendix 1) employed dichotomous, multiple choice, multi-select, and Likert scale questions and covered topics such as symptom recognition for laryngeal cancer, confidence in diagnosis, misconceptions about post-laryngectomy capabilities, and interest in further educational resources.
Following data collection, statistical analysis was performed using SPSS v26. Descriptive statistics were calculated to summarize physician responses to Likert scale and dichotomous questions. Incomplete surveys were excluded from analysis.
Results
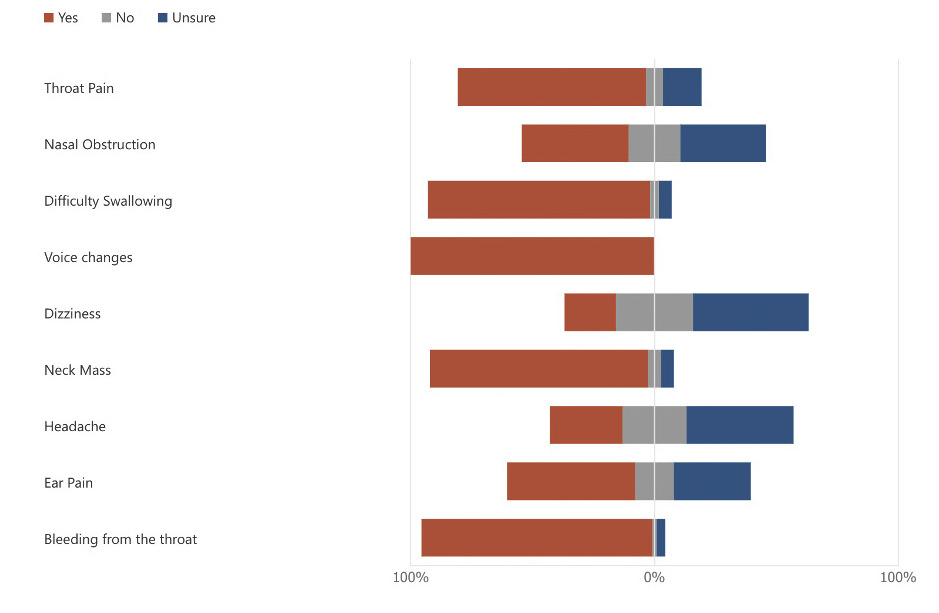
Fifty-seven PCPs completed the survey in its entirety, with a response rate of 10.5%. When asked if the providers were confident in identifying early signs of laryngeal cancer 35.1% of participants were neutral, 29.8% agreed, 22.8% disagreed, 7.0% strongly agreed, and 5.3% strongly disagreed. Examining symptom recognition (Figure 1), all participants identified voice changes as a symptom of laryngeal cancer, but only 52.6% recognized ear pain as a potential symptom. Most recognized throat pain as a potential symptom (77.2%), as well as difficulty swallowing (91.2%), presence of a neck mass (89.4%), and bleeding from the throat (94.7%). Most were unsure whether dizziness (47.4%) and headache (43.9%) were symptoms of laryngeal cancer, and 43.9% stated that nasal obstruction could be a presenting symptom. When asked if stridor was a sign of early laryngeal cancer, 42% incorrectly answered ‘true.’

A majority of participants agreed that patients diagnosed with laryngeal cancer should be referred to a tertiary care center and ultimately be presented at a multidisciplinary tumor board to determine treatment recommendations (43.9% strongly agreed, 40.3% agreed). Regarding referral timing, 47% indicated persistent hoarseness should prompt ENT referral after three weeks, followed by six weeks (44%), and one week (9%), with no respondents selecting nine weeks. For a 50-year-old with a persistent neck mass, 49% reported referral after two rounds of antibiotics, with 44%, 5%, and 2% selecting referral after one, three, and four rounds, respectively.
When asked about barriers affecting their ability to make an appropriate referral for laryngeal cancer, the most common answer was provider skill in screening assessment (24.4%), followed by provider knowledge of early warning symptoms (22%), patient insurance status (20.5%), patient inability to recognize early symptoms (16.5%), unsure about referral options and unsure where to refer with 10 responses each (7.9%), and one participant responding other (0.8%). When asked about what would help improve referral capacity for laryngeal cancer, the most common selection was brochures or education materials (35.4%), followed by distance learning module (25.6%), do not need any help (14.6%), hands-on skill training (13.4%) and 1 participant indicating other (1.2%).
Regarding smoking cessation counseling, 78.9% of participants were aware that they could bill for smoking cessation counseling during an office visit, and the majority of providers agreed (28.1% strongly agreed, 38.6% agreed) that being able to bill for smoking cessation counseling would encourage them to spend time on such counseling during office visits. Forty-seven responders (82%) stated they counsel patients very often on smoking cessation. More than half of the participants surveyed (57.9%) indicated they had concerns about adding additional screening and counseling time to their exams, with the concern most often being related to time constraints (49.3%). When asked if it is important to screen tobacco users for symptoms of head and neck cancer, 59.7% of participants strongly agreed, while 26.3% agreed, 3.5% were neutral, and 10.5% strongly disagreed.
Most providers (92.9%) agreed that there could be advantages to adding laryngeal cancer screening to appropriate patient exams (36.8% strongly agreed, 56.1% agreed), and that participating in an educational program about the warning signs of head and neck cancers would ultimately have a positive impact on their practice (26.3% strongly agreed and 43.9% agreed). Additionally, 77.2% of participants indicated they would participate in such a program if continuing medical education (CME) were offered. When asked what would make them more likely to implement head and neck cancer screening into their practice, the most common answer was standardized screening tool (45%), followed by patient information brochures (19.2%), online education modules with CME credit (14.2%), further information on how to implement screening (13.3%), and in-person education with CME credits (7.5%). One participant (0.8%) indicated they were unlikely to implement screening. When asked how likely they would be to use a validated screening tool for laryngeal cancer, most indicated very likely (51%) or somewhat likely (39%).
Discussing laryngectomy patients, only 42.1% of respondents knew that patients could speak after laryngectomy; however 82.4% correctly responded that the statement “patients are unable to swallow after laryngectomy” is false, while 8.8% were unsure and 8.8% answered incorrectly.
Discussion
Access to primary care is linked with better health outcomes, reduced healthcare costs, and fewer hospital admissions.15–17 As PCPs are often the initial point of healthcare contact, they play a critical role in guiding patients through the healthcare system and ensuring timely referral to specialty care. Prior studies demonstrate that continuity with a PCP is associated with earlier cancer diagnosis and reduced cancer-specific mortality.8,18–20 In laryngeal cancer specifically, prompt detection and referral are essential, as delays in diagnosis are closely linked to worse prognosis.3 A retrospective cohort study in the United Kingdom found that laryngeal cancer ranked among the cancers with the longest interval between diagnosis and primary care referral.21 Shephard, et al., demonstrated increased PCP visits in the year preceding laryngeal cancer diagnosis.22 Our results demonstrate variability in referral thresholds for persistent hoarseness and neck mass, with many providers delaying referral beyond three weeks or requiring multiple antibiotic trials. These practices likely contribute to delays in diagnosis and specialty referral.
A lack of formal otolaryngology training in medical education may contribute to delayed otolaryngology referrals. Despite PCPs reporting otolaryngic issues as relevant to daily practice,23,24 multiple studies have demonstrated limited otolaryngology exposure during medical school and postgraduate medical education.7,9–14 Consistent with this finding, only 36.8% of our surveyed providers felt confident identifying early signs and symptoms of laryngeal cancer. While most providers recognized common symptoms such as voice changes and throat pain, fewer identified otalgia, and many incorrectly associated non-specific symptoms such as headache and dizziness. Additionally, 42% incorrectly identified stridor as an early sign of laryngeal cancer. These findings highlight persistent gaps in symptom recognition and reinforce the need for targeted laryngeal cancer education within primary care.
Tobacco use is a major risk factor for the development of head and neck cancer but also has a significant detrimental impact on prognosis with poorer survival noted in current smokers compared to former smokers and never smokers.25 The World Health Organization argues that primary care is the most suitable setting for advice and support for smoking cessation due to more frequent opportunities to identify use and help patients quit.26 However, many PCPs are not providing this service, as many of them have not received training in delivering specific interventions.27 In our survey, 82% of responders stated they very often counsel patients on smoking cessation, with 79% aware they can also bill for that service. This figure is higher than previously reported literature demonstrating suboptimal PCP adherence to cessation guidelines, with less than 50% of PCPs offering support to patients.27 The higher relative rates observed in our study may reflect the fact that the surveyed providers practice in a state where tobacco use exceeds the national average.28 Nonetheless, these findings highlight the importance of continued education on smoking cessation counseling to support prevention efforts.
The present study highlights an opportunity for continuing medical education (CME) initiatives. Previous studies have shown that PCPs are interested in further education in otolaryngology,7,13 and 77% of respondents in our study reported willingness to participate in an educational program focused on early warning signs of laryngeal cancer if CME credit were offered. CME has been shown to improve patient outcomes and influence practice changes.29,30 Cancer-specific educational initiatives in skin, prostate, colorectal, pediatric, breast, and ovarian cancers have demonstrated improvements in provider knowledge, diagnostic confidence, and referral practices.31–36 Additionally, Del Poggio, et al., demonstrated that an educational program for PCPs led to increased early-stage detection and improved 5-year survival in hepatocellular carcinoma.32 Prior studies also demonstrate the utility of head and neck cancer screening programs in high-risk populations,37–39 underscoring the potential impact of structured educational approaches on early cancer detection.
Most providers in this study also expressed interest in additional education and resources related to laryngeal cancer, and many indicated they would be likely to use a validated laryngeal cancer screening tool if available. Although a validated laryngeal cancer screening tool does not currently exist, survey findings informed the development of an online educational program for Mississippi primary care physicians focused on early recognition and referral of suspected laryngeal cancer. This program is grant-funded for two years and incorporates pre- and post-education surveys to assess its impact on provider knowledge, confidence, and referral practices. By equipping PCPs with targeted knowledge, this initiative aims to support earlier identification and ENT evaluation of patients with symptoms concerning for laryngeal cancer.
Limitations to this study include response rate of 10.5%, which may introduce response bias. Additionally, surveys were distributed in counties with the highest incidence of laryngeal cancer, potentially increasing baseline awareness among respondents. As this survey was aimed to collect information for future educational initiative, provider demographic characteristics were not collected, limiting subgroup analysis of provider demographics or training background.
Conclusions
This study highlights the current challenges in primary care regarding management and referral of patients with otolaryngic symptoms concerning for head and neck cancers and specifically laryngeal cancer. These findings underscore the need for targeted educational interventions to improve knowledge in providers serving in Mississippi and other areas with high risk populations. PCPs were overwhelmingly interested in engaging in further education on laryngeal cancer.