




Let This Sink in: Enophthalmos as a Rare Presentation of Lobular Breast Carcinoma
Case presentation
A 74-year-old female presents with 10 months of unilateral restricted extraocular movement, progressive narrowing, and right periorbital pain. Further examination revealed enophthalmos, esotropia, upward gaze palsy, hypotropia, decreased visual acuity, and normal ocular pressure of the right eye. The initial ocular presentation was believed to be secondary to her uncontrolled diabetes mellitus; however, since this presentation is not typical, the patient required further workup. Additionally, the patient reported her last mammogram revealed a cystic lesion in her left breast confirmed with ultrasound.
Images
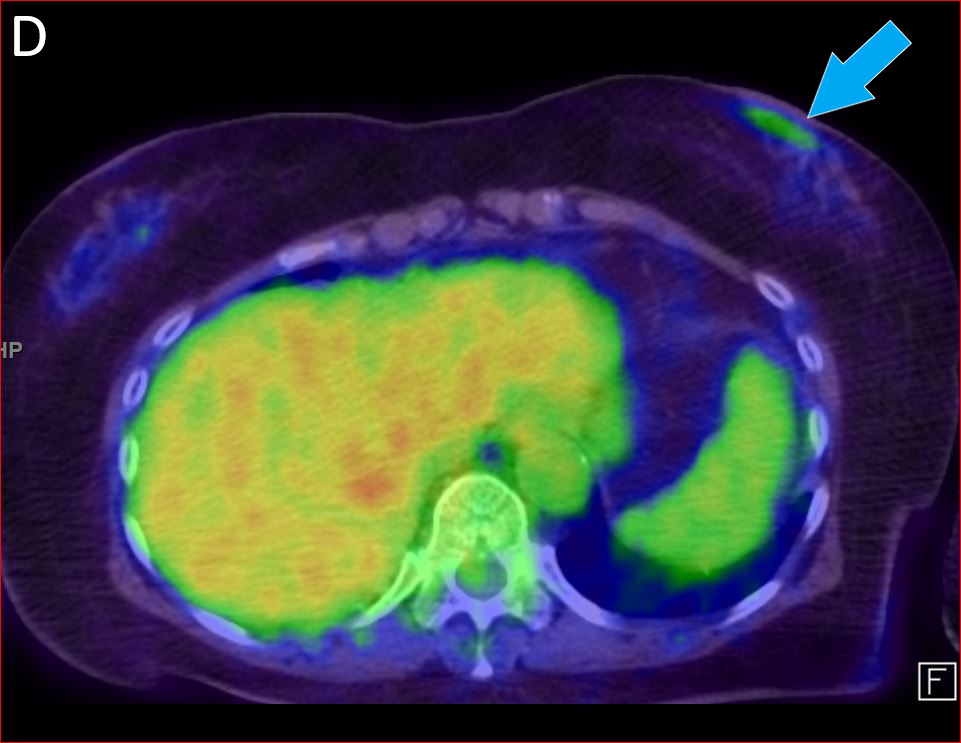
Figure A, coronal CT of the orbits demonstrates infiltrative, enhancing soft tissue in the right orbit (red arrow), predominately intraconal. Figure B, axial CT of the orbits demonstrates the infiltrative enhancing mass in the right orbit which causes enophthalmos (white arrow) compared to the normal left side. Figure C, coronal reformat PET overlaid on the CT orbits which demonstrates abnormal uptake in the right orbit (orange arrow) corresponding to the infiltrative soft tissue mass. Figure D, axial PET/CT demonstrates low-level abnormal uptake in the left subareolar breast (blue arrow). Figure E, clinical photograph demonstrating the enophthalmos and bruising of the right periorbital soft tissues.




Discussion
The patient was referred to ophthalmology for multiple cranial nerve palsies affecting the right eye, and computed tomography (CT) of the orbit revealing an infiltrative mass encasing the posterior right globe and optic nerve with invasion to the preseptal right orbit. The biopsy of the mass was consistent with metastatic invasive lobular carcinoma (ILC) of the breast. Further evaluation of primary and metastatic disease with a follow-up 18F-fluorodeoxyglucose positron emission tomography (FDG-PET)/CT scan showed a mildly hypermetabolic right orbital mass and very low-level uptake in the subareolar left breast. Of note, ILC does not avidly take up FDG, limiting the sensitivity.1 Furthermore, imaging alone is not adequate to diagnose the etiology of the tumor, as radiological findings of orbital tumors may overlap.2
Invasive ductal carcinoma (IDC) and ILC account for roughly 75% and 10% of primary breast malignancies, respectively.3 Compared to IDC, ILC presents at later stages with more distant metastases.4 Enophthalmos occurs most commonly in desmoplastic variants of IDC (scirrhous breast carcinoma) but has also been reported with ILC.5 While metastatic disease to the orbit is rare, constituting 1 to 13% of orbital tumors,6 breast cancer is the most frequent primary source, accounting for 29-53% of cases,3 with other less common sources from the prostate, lung, gastrointestinal tract, skin, and parotid gland.6 The prognosis of orbital metastasis of primary ILC is very poor with survival running from 1 to 116 months with a mean of 31 months.3 Recommended management for this patient is palliative care with treatment options including systemic chemotherapy, hormone therapy, orbital radiotherapy, or any combination thereof. Surgery can also be used as a diagnostic modality or for further palliative care.3 The patient reported completion of radiation therapy and current therapy with palbociclib and letrozole.
In conclusion, while ILC is a rare variety of metastatic cancer, it is associated with significant morbidity.3 Healthcare professionals must keep clinical suspicions high for metastatic breast carcinoma to the orbit when enophthalmos is present and provide a comprehensive clinical assessment.
Acknowledgments
Additional informed consent was obtained from all individuals for whom identifying information is included in this article.
ALT is President of the Mississippi Society of Nuclear Medicine.
CST is Mississippi state representative of the Radiology Advocacy Network and chair of the membership committee of the Association of Program Directors in Radiology.