
Introduction
The United States (US) has the highest maternal mortality rate (MMR) among industrialized nations.1 Although MMRs in the US are high in general, data from the 2021 National Vital Statistics System showed non-Hispanic Black Americans (69.9 per 100,000 live births) were disproportionally impacted relative to White Americans (26.6 per 100,000 live births) and women of all races and ethnicities (32.9 per 100,000 live births).2 Furthermore, MMRs and racial disparities are persistently high in the Southeastern US.3 In particular, the 2018-2021 MMRs were among the highest in Arkansas (43.5 per 100,000 live births; ranked highest), Louisiana (39.0 per 100,000 live births; ranked 5th highest), and then Mississippi (43.0 per 100,000 live births; ranked 2nd highest).4,5 More than 80% of maternal deaths occurring during pregnancy or within 12 months postpartum are preventable; most of these preventable deaths are related to maternal mental health disorders.6,7
The National Institutes of Health launched the IMPROVE initiative in 2019 to support research on the preventable causes of maternal morbidity and mortality (MMM). In 2023, the Southern Center for Maternal Health Equity (SCMHE) was established with funding from the IMPROVE initiative to reduce MMRs and racial disparities in the Southeast.8 There are three distinct seven-year NIH grant-funded research studies supported under the SCMHE with the overarching aim of assessing the implementation and translation of multi-level, evidence-based strategies to improve maternal health. One of these studies is evaluating the effectiveness and cost-effectiveness of Medicaid postpartum coverage extension (MPE) and postpartum depression screening on maternal health outcomes in the Deep South.
The American Rescue Plan Act of 2021 allowed states the option to extend postpartum coverage from the mandated 60 days to up to 12 months post-delivery.9 Louisiana was the first state to approve MPE in 2022,10 and Mississippi followed in 202311; however, as of 2024, Arkansas has not sought MPE. In 2022, Louisiana legislation also mandated screening for postpartum depression.12 Evidence suggests that state legislation can potentially improve maternal health and reduce racial disparities in MMR.13 SCMHE investigators and community partners conducted retrospective surveillance of enacted legislation in Arkansas, Louisiana, and Mississippi between 2018 and 2023 to provide context for studying the impact of MPE and other relevant policies on maternal health. This descriptive report summarizes the legislation enacted within these three Southeastern states where MMRs are among the highest nationally. The findings provide a contextual foundation for understanding the impact of MPE and other maternal health policies on maternal health outcomes.
Methods
The Maternal and Child Health Legislative Database, operated by staff of the National Conference of State Legislators (NCSL), tracks legislation of interest to the maternal and child health population.14 The NCSL is a non-partisan entity. As noted on their website, it is maintained with support from the Maternal and Child Health Bureau of the Health Resources and Services Administration and only covers legislation enacted into law.
The study team searched the NCSL database for all legislation relating to maternal health in Arkansas, Louisiana, and Mississippi between 2018 and 2023. Inclusion criteria followed PICO (population, intervention, comparator, outcome). The population of interest included pregnant, peripartum, and postpartum women within 12 months of delivery. Policy (interventions) were included if there was a directive impacting maternal health, well-being, or health care. Health outcomes were not restricted; legislation was included if the directive was tied to health issues such as maternal mental health, breastfeeding, long-acting reversible contraceptive insertion, clinical screening, and procedures or processes impacting public or clinical health care. Comparators are not applicable in this surveillance report. The search for eligibility and inclusion was carried out independently by two reviewers (SA and UN). The reviewers then conferred and cross-checked the legislation identified by year and state. Any disagreements were resolved through discussion based on the PICO outlined until consensus was reached.
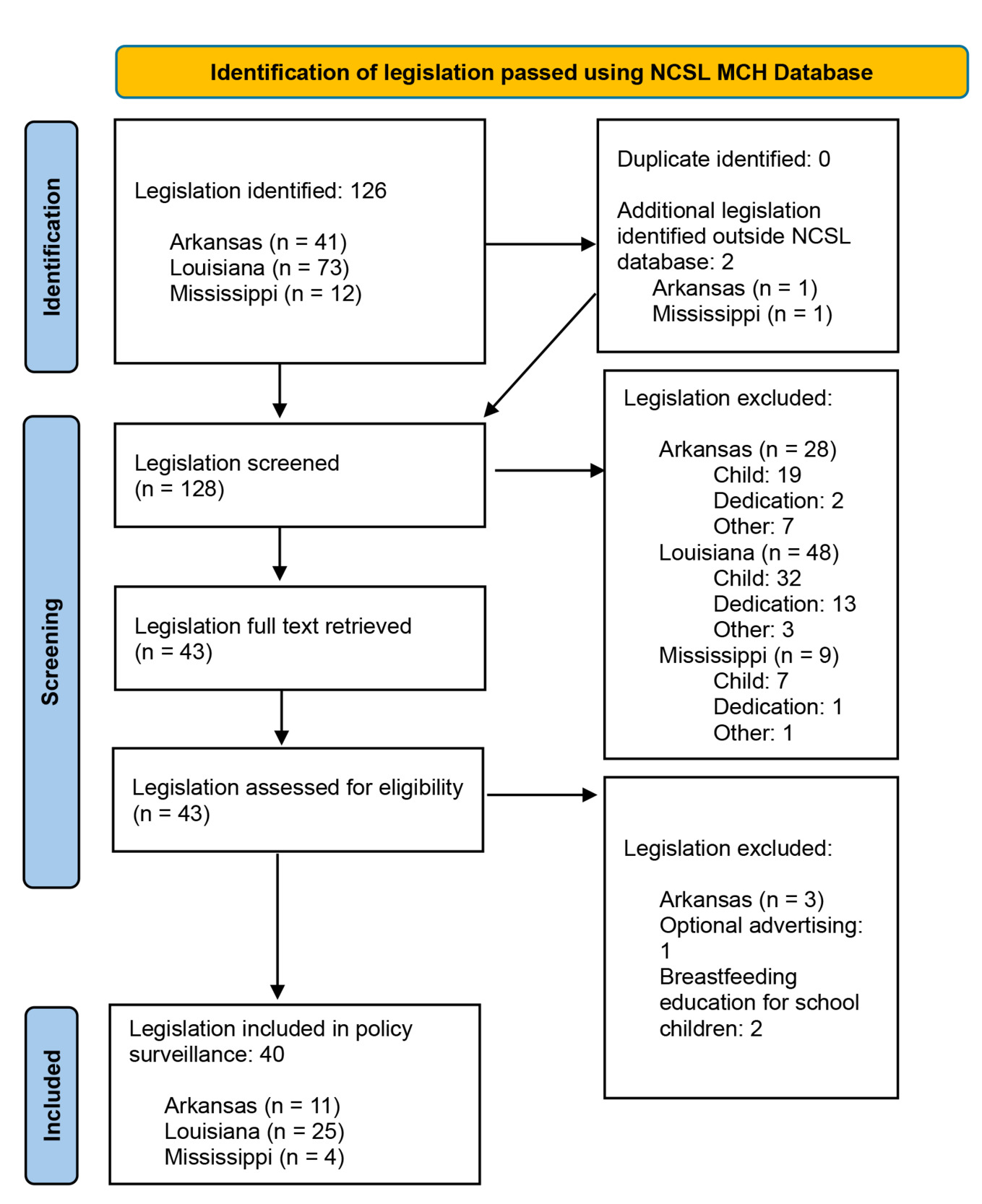
The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement provides guidelines and a checklist for the conduct of systematic reviews. In the absence of reporting guidelines for policy surveillances such as this effort, the screening process has been documented using a modified PRISMA diagram.15 The use of the PRISMA workflow ensures reproducibility and details key processes required to document the methodology, rigor, and systematic nature of this surveillance of legislation. The date of the last search was 15th March 2024.
The data extracted included the year and state in which the law was enacted, the legislative house, the bill number, the act number (if applicable), the target population, the general topic of the bill, and the directive. If a bill pertained to more than one item in its summary, only the portion pertinent to maternal health was extracted. Data extraction was carried out by SA and verified by UN and AG.
Results
Between 2018 and 2023, 126 legislations were enacted in Arkansas, Louisiana, and Mississippi; 40 of those were related to maternal health. Most (n=25; 62.5%) bills were passed by the Louisiana legislature, followed by Arkansas (n=11; 27.5%) and Mississippi (n=4; 10.0%). Figure 1 shows the screening process using the modified PRISMA diagram, stratified by state.15
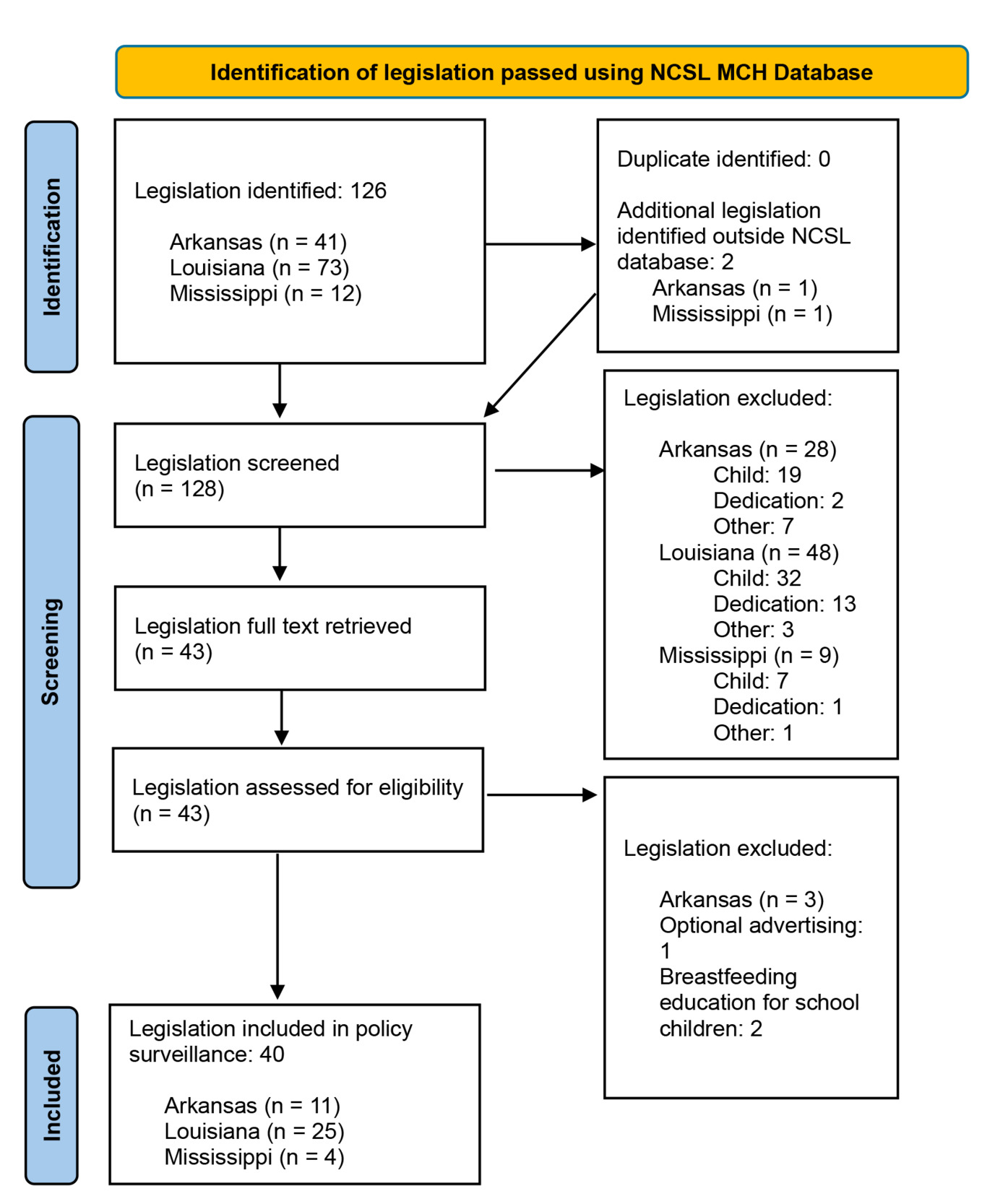
Table 1 describes the target population, health topic, and directive of each bill by state and year.
Populations
Most legislation targeted general pregnant and postpartum populations (n=22; 55.0%). Nine bills were related to Medicaid (22.5%), six targeted incarcerated persons (15.0%), two were related to adolescents (5.0%), and one was specific to rural populations (2.5%).
Health Topic
Twelve (28.6%) bills addressed general maternal health and well-being. Seven (16.7%) bills sought to improve maternal mental health, six (14.3%) were related to breastfeeding or human donor milk, five (11.9%) addressed MMM, and five (11.9%) pertained to increasing services covered by Medicaid. Two bills each sought to reduce abortion (4.8%), improve labor and delivery outcomes (4.8%), and increase access to long-acting reversible contraception (4.8%). Timely and evidence-based treatment of substance use in pregnant and postpartum women was the health topic of one bill (2.4%).
Directives
There were 42 directives set by the enacted legislations; two of the 40 laws had multiple directives. Insurance coverage was the most common directive with 13 laws (31.0%) addressing either Medicaid coverage or other forms of insurance coverage. Five laws (11.9%) created advisory councils or task forces, and five (11.9%) formed a review committee, study commission, or mandated an audit. Four laws (9.5%) were related to health care or clinical treatment, and four (9.5%) established a policy: for example, high school attendance and breastfeeding policies for adolescents. Two laws (4.8%) in Louisiana requested that racial disparities in MMM be addressed, two (4.8%) mandated staff training in maternal health care, and two (4.8%) required information resources be developed and made available to pregnant populations and their families. The remaining five laws (11.9%) sought to create clinical-community linkages, conduct a pilot study, assess health care utilization, establish licensure for maternal support service providers, and form a doula registry.
Narrative Summary
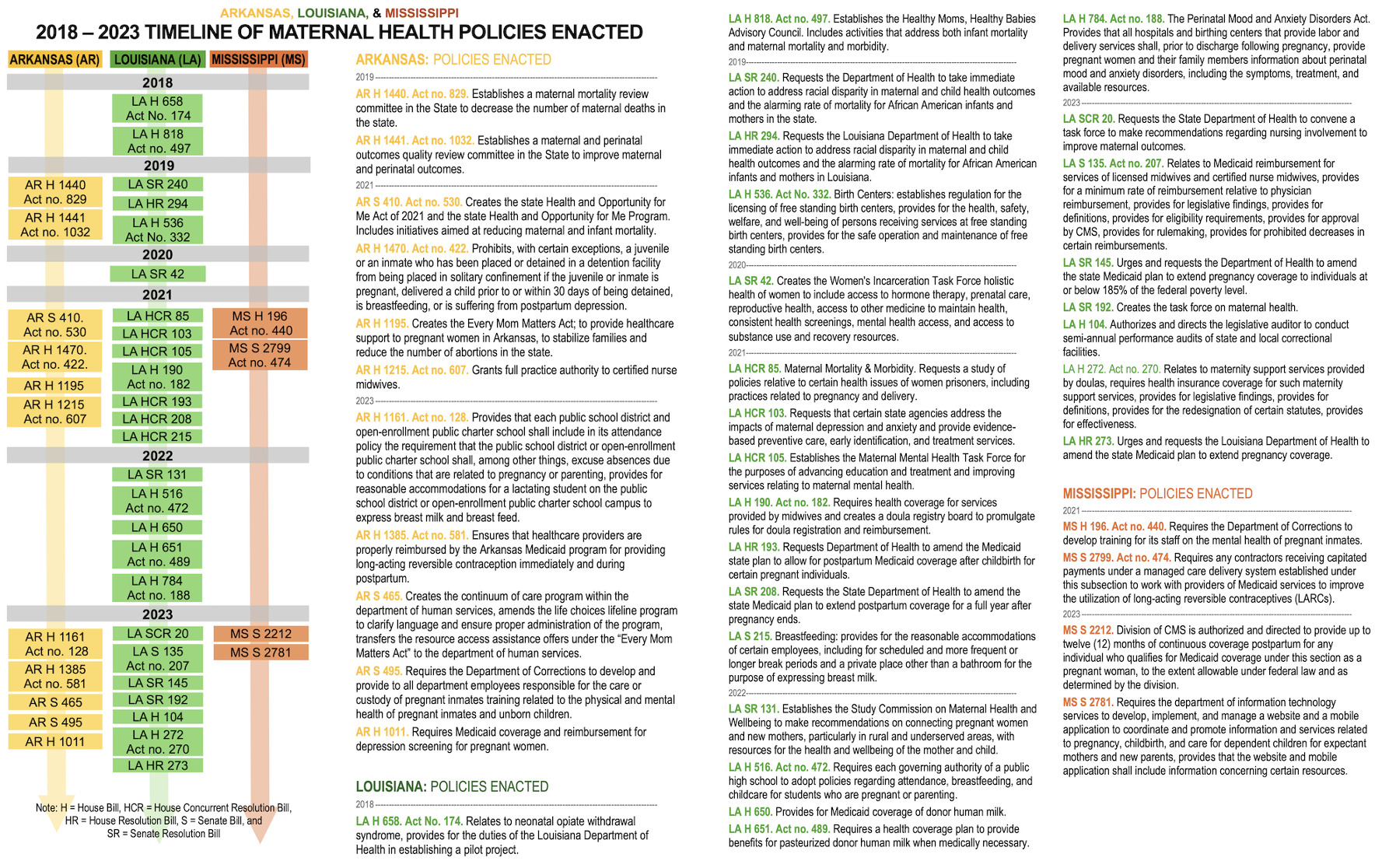
An infographic of the laws included in this report is shown in Figure 2.
Maternal morbidity and mortality
In 2018, Louisiana established the Healthy Moms, Healthy Babies Advisory Council to address MMM. The council’s charge included studying maternal health disparities by race and ethnicity, evaluating activities, collaborating with maternal health organizations and entities, and advising on policy options to eliminate preventable MMM. In 2019, Louisiana passed additional legislation to address disparities in MMM. This directive was to take action to implement measures to combat this crisis, including requiring health care diversity sensitivity training and increasing access to home visits and doulas.
In 2023, the legislature requested that the Louisiana State Nurses Association create the Nursing Maternal Mortality and Pre-term Birth Task Force to make recommendations on how nurses can improve MMM and, separately, mandated the creation of a Task Force on Maternal Health to study strategies to improve health outcomes.
In 2019, Arkansas established a Maternal Mortality Review Committee and a Maternal and Perinatal Outcomes Quality Committee to decrease MMM, and, in 2021, enacted the Health and Opportunity for Me Act (ARHOME), which included initiatives to reduce MMM.
Incarcerated populations
In 2020, Louisiana established the Women’s Incarceration Task Force to promote holistic health approaches including access to hormone therapy, prenatal care, mental health support, and substance use recovery resources. Following this effort, in 2021, the Louisiana legislature requested a study of health policies for female prisoners, including issues of pregnancy and delivery. Another law passed in 2023 mandated performance audits of state and local correctional facility compliance, implementation, and enforcement of prior Acts on the use of restraints and solitary confinement of pregnant women.
In 2021, Arkansas enacted protections prohibiting juveniles or inmates from being placed in solitary confinement if they were pregnant, within 30 days postpartum, breastfeeding, or diagnosed with postpartum depression. That same year, Mississippi required the Department of Corrections to develop training for its staff on the mental health of pregnant inmates. In 2023, Arkansas also charged the Department of Corrections to provide physical and mental health training to all employees in the custody of, or providing care for, pregnant inmates.
Medicaid
In 2021, a House and a Senate bill were passed that requested the Louisiana Department of Health (LDH) to amend the state plan for MPE to 12 months, which was later approved in 2022 by the Centers for Medicare and Medicaid Services. Additionally, in 2023, Louisiana passed a House and a Senate bill urging and requesting that LDH amend the state Medicaid plan to extend pregnancy coverage from 138% of the federal poverty level to 185%.
In 2023, Mississippi adopted MPE for up to 12 months postpartum. Before this date, in 2021, Mississippi authorized capitated payments under Medicaid-managed care delivery systems to increase the use of long-acting reversible contraceptives. Arkansas established Medicaid long-acting reversible contraceptives reimbursement legislation in 2023.
Mental Health
In 2021, Louisiana established the Maternal Mental Health Task Force to advance education, treatment, and services related to maternal mental health, and, in a separate bill, requested the LDH and medical community provide evidence-based preventive care, screening, and treatment services. In 2022, Louisiana mandated information and resources about perinatal mood and anxiety disorders be disseminated to women prior to hospital discharge. The Louisiana legislature also mandated the Study Commission on Maternal Health and Wellbeing to make recommendations for connecting pregnant and postpartum women in rural and underserved areas to health resources.
In 2021, Arkansas amended the Life Choices Lifeline Program to include mental health care for depression and substance use disorders, and in 2023, it required Medicaid coverage for depression screenings.
Breastfeeding and donor human milk
In 2021, the Louisiana legislature required employers to make accommodations for breastfeeding, including scheduled and more frequent or longer break periods and a private place other than a bathroom to express breast milk. Louisiana also passed measures on donor human milk coverage in health plans and breastfeeding and childcare policies in public high schools for students. Arkansas passed a similar law in 2023 requiring public schools and open-enrollment public charter schools to accommodate breastfeeding, expressing milk, and absences related to pregnancy or parenting.
Midwives and doulas
To enhance maternal health care in 2021, Louisiana required health care coverage among private insurers for midwifery services and established a doula registry board. Similarly, Arkansas granted full practice authority to certified nurse midwives. In 2023, Louisiana requested Medicaid and other health insurance coverage for support services provided by doulas.
Discussion
This retrospective surveillance report describes the policy landscape of maternal health legislation in Arkansas, Louisiana, and Mississippi between 2018 and 2023. The Louisiana legislature enacted the most laws, including approval for MPE and other legislation that has sought to address racial disparities and provided considerations for special populations (e.g., incarcerated persons and adolescent mothers). Mississippi enacted the fewest bills; however, approval for MPE in 2023 was a critical milestone for the state. While Arkansas has not sought MPE, the state legislature has demonstrated support for maternal mental health improvement, breastfeeding accommodations, and midwives and doulas.
Only two bills, both in Louisiana, overtly gave the directive to engage community partners or take regulatory action to address racial disparities, specifically among Black or African American mothers. Developing a diverse perinatal workforce, including midwives and doulas, is a key strategy to reduce racial disparities.16 Studies have shown that among Medicaid beneficiaries, women whose labor and delivery were supported by a doula had improved birth outcomes and rates of breastfeeding initiation.17 Given that Medicaid covers more than 60% of births among Black mothers,16 increasing legislation to support their role may further reduce racial disparities in maternal health outcomes.18 In Louisiana, legislation enacted to support training doulas and midwives in conjunction with Medicaid mandates to reimburse for services is a promising multi-component approach to advance reproductive justice among Black women in the state.
Louisiana also led the charge among the three states in promoting maternal mental health. Postpartum depression is the most common and preventable maternal health complication following childbirth.6 Despite recommendations made by the US Preventive Services Task Force19 and the American College of Obstetrics and Gynecology,20 clinical screening, treatment, and prevention practices are lacking.21,22 Research and policy development are needed to improve the availability and accessibility of mental health prevention and treatment services.23 The SCMHE will assess the effectiveness of Louisiana’s Perinatal Mood and Anxiety Disorders Act (HB784, Act 188; 2022) on screening and treatment of mental health disorders among Medicaid beneficiaries, in comparison to Mississippi and Arkansas, where screening practices are not mandated.
A final point of discussion on abortion trigger laws is warranted. In June 2022, the Supreme Court of the United States in its decision in the Dobbs v. Jackson Women’s Health Organization case overruled Roe v. Wade and ended the constitutional right to abortion.24 The power to prohibit or limit abortions was returned to the states. Trigger laws in Arkansas (AR SB 149, Act number 180; 2019), Louisiana (LA SB 33, Act number 467; 2006), and Mississippi (MS SB 2391; 2007) went into effect soon after the 2022 Supreme Court decision, with a few state-based exceptions such as medical emergencies or rape. A potential unintended consequence of restrictions on abortion may result in increased racial disparities in MMM.25,26
Limitations
There are several limitations to this report. First, the results were based on a single database and may be limited by the legislation tracked by the NCSL. For example, Mississippi SB 2212, which approved MPE, was not included in the Maternal and Child Health database. Arkansas’ 2023 amendment of the Life Choices Lifeline program to create the Continuum of Care Program was included (S 465) in the database, but the 2021 amendment, Every Mom Matters Act (H 1195), was not. Second, screening only the bill title and summary to select legislation for full-text review may have excluded relevant bills. For example, Louisiana’s 2018 bill on neonatal opioid withdrawal syndrome (H 658) did not mention maternal priorities in the title and summary; however, a full-text review revealed maternal access to evidence-based treatment for substance use disorder as one of its priorities. Another limitation was that this retrospective surveillance included enacted legislation only. Bills introduced but not passed demonstrate impetus for improving maternal health, which is important to understanding context. Finally, guidelines for conducting rigorous and reproducible policy surveillance have not been developed.
Population health implications
This is one of the few retrospective surveillance reports of enacted maternal health legislation available in the scientific literature. Findings from this report provide the SCMHE investigators and community partners with an understanding of the historical context for legislation to improve maternal health and reduce MMM and racial disparities in Arkansas, Louisiana, and Mississippi. The next steps are to examine the effectiveness and cost-effectiveness of MPE (Louisiana, Mississippi) and mental health screening mandates (Louisiana) on maternal health outcomes, as compared to counterparts in Arkansas. Longitudinal surveillance of proposed and enacted legislation across these three Southeastern states is ongoing and will contribute to our understanding of policy impacts on MMM and maternal health equity.
Funding/Support
This work is funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (U54HD113159).
Disclaimer
Utsav Nandi serves on the editorial board of the JMSMA but was not involved in any of the decisions regarding review of the manuscript or its acceptance.