Case Presentation
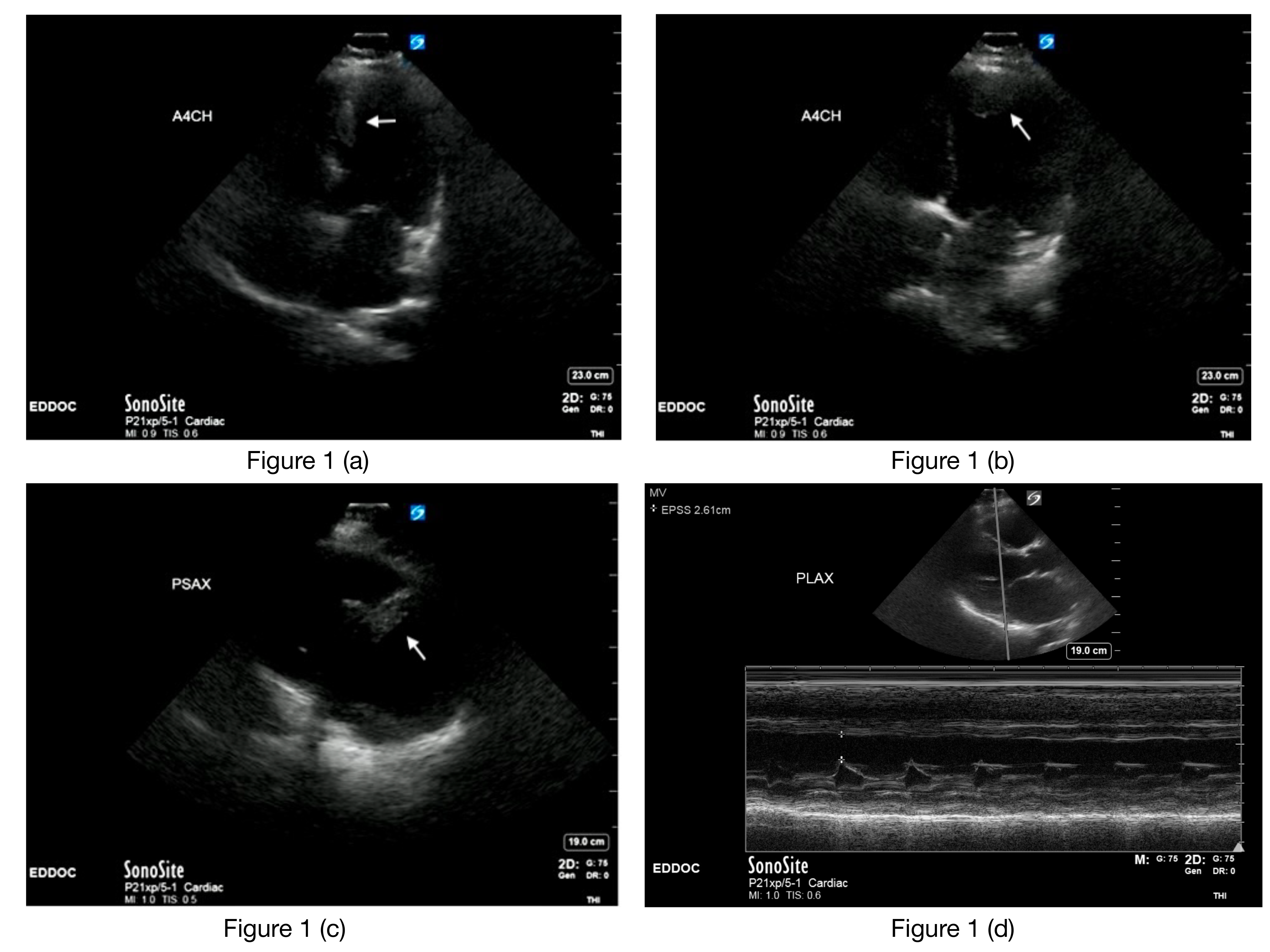
A 58-year-old male with a past medical history of hypertension and diabetes mellitus type II presented to the Emergency Department (ED) for evaluation of worsening shortness of breath and bilateral lower extremity swelling. He was evaluated at a local clinic for these symptoms three weeks prior and advised to start taking Lasix 40 mg daily and follow up with Cardiology in six weeks. He notes some associated intermittent mid-sternal chest pressure and a 30-lb weight-gain over this time. Initial vitals on presentation: BP 127/93, HR 116, RR 22, O2 saturation 99% on room air. His physical exam was notable for 2+ pitting edema to bilateral lower extremities. Labs were notable for a troponin T of 0.07 ng/ml and proBNP of 6,727 pg/ml. Point of care ultrasonography (POCUS) was performed to evaluate his cardiac function, and the images are shown in Figure 1.
_apical_4-chamber_(b)__apical_4-chamber_(c)_parasternal_short_axis_(d)_m-mo.png)
Discussion
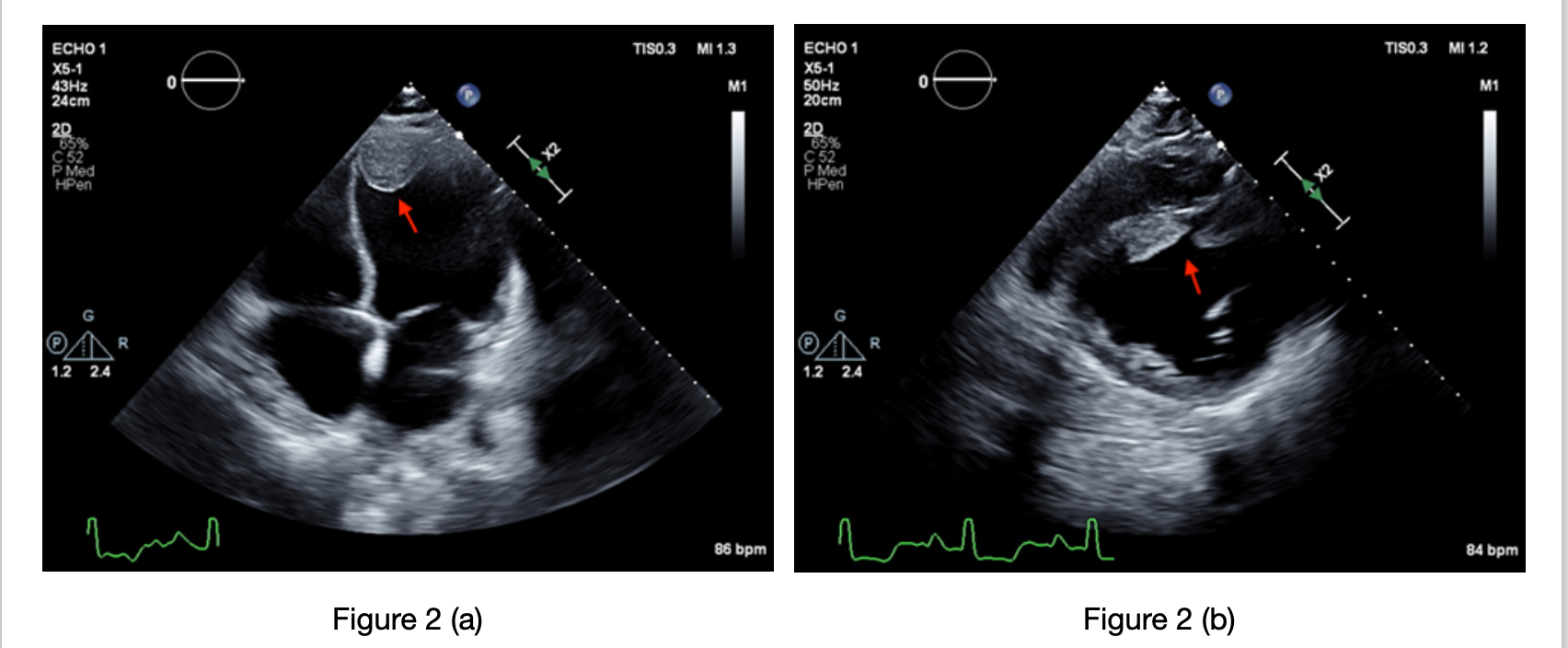
POCUS showed echogenic areas of concern (figures 1a, 1b and 1c) and significantly reduced left ventricular (LV) function by visual estimation and by abnormal E-point septal separation (figure 1d). Due to concern for an LV thrombus, newly diagnosed heart failure, and an NSTEMI, he was started on heparin and diuretics in the ED in consultation with cardiology, and he was admitted to their service for inpatient management. Inpatient echocardiogram showed an ejection fraction of <15% and confirmed two LV thrombi (figure 2a and 2b), the largest measuring 3.35 x 2.8 cm. Left heart catheterization showed disease in the left anterior descending (LAD) and right coronary artery. He subsequently underwent stenting of the LAD and was started on aspirin and clopidogrel. Following optimization of his newly diagnosed heart failure, he was bridged to warfarin for management of his LV thrombus and discharged with Cardiology follow-up.
_apical_4-chamber_(b)_parasternal_short_axis.png)
LV thrombi typically develop as a complication following an acute myocardial infarction (MI) and, less frequently, the development of dilated cardiomyopathy (DCM).1 The incidence of LV thrombus associated with acute MI or DCM ranges anywhere from 2% to 39% and is associated with up to a 22% risk of embolization.2 The apical kinesis and/or wall motion abnormalities that can accompany an MI, or the diminished systolic function that can accompany dilated cardiomyopathy, create a favorable environment for Virchow’s triad of stasis, endocardial damage, and hypercoagulability, predisposing the patient to development of an LV thrombus.3 The potential of these thrombi to embolize and cause a stroke or ischemia to vital organs makes prevention, early diagnosis, and management important. Traditionally, a Vitamin K antagonist (VKA) like warfarin has been used to treat LV thrombi. However, recent literature also indicates that direct oral anticoagulants are safe alternatives to VKAs.2
Point-of-care cardiac ultrasound (POCUS) has become an indispensable tool for rapid diagnosis and intervention in the emergency department and its diagnostic utility continues to expand.4 While it is increasingly being used to assess cardiac function in the ED, this case also illustrates its utility in detecting rarer pathology that can help clinicians start prompt treatment and facilitate appropriate referrals.